

Echinococcosis is a zoonotic disease caused by the genus Echinococcus. Echinococcosis occurs in 4 forms: 1) cystic echinococcosis caused by Echinococcus granulosus (E. granulosus); 2) alveolar echinococcosis caused by E. multilocularis; 3) polycystic echinococcosis caused by E. vogeli; 4) unicystic echinococcosis caused by E. oligarthrus. The two most important forms in humans are cystic and alveolar echinococcosis.
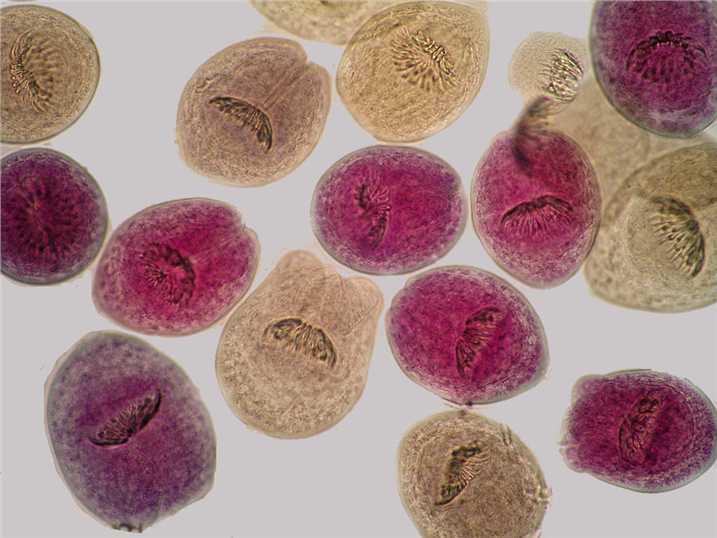
Human infection with E. granulosus leads to the development of one or more hydatid cysts located most often in the liver and lungs, and less frequently in the bones, kidneys, spleen, muscles and central nervous system. When hydatids occur in the liver, abdominal pain, nausea and vomiting are commonly seen. If the lung is affected, chronic cough, chest pain and shortness of breath may occur. Other signs depend on the pressure exerted on the surrounding tissues and the location of the hydatid cysts. Non-specific signs include weight loss and weakness.
There is an asymptomatic incubation period of 5-15 years after E. multilocularis infection. The slow development of a primary tumor-like lesion is usually located in the liver. Clinical signs include abdominal pain, weight loss, general malaise and signs of hepatic failure. Larval metastases may spread either to organs adjacent to the liver or distant locations following dissemination of the parasite via the blood and lymphatic system. If left untreated, alveolar echinococcosis is progressive and fatal.
For both cystic echinococcosis and alveolar echinococcosis in humans, ultrasonography imaging technique is a good choice. Computed tomography (CT) and magnetic resonance imaging (MRI) scans are usually recommended for further validation. Cysts can be incidentally discovered by radiography. Specific antibodies are detected by different serological tests and can support the diagnosis. Early detection of E. granulosus and E. multilocularis infections is still needed for the selection of clinical treatment options.
Cystic echinococcosis in humans has considerably been controlled by an efficient and effective vaccine, which indirectly prevents humans from infection. The vaccine protects animal intermediate hosts, thus the lack of hydatid cysts in these animals will prevent dogs to become infected, which on the long-term will result in an abrogation of infection sources for humans and other intermediate hosts.
It is often expensive and difficult to treat both cystic echinococcosis and alveolar echinococcosis. Sometimes, extensive surgery and prolonged drug therapy are needed. Surgical removal of the cysts is the most common treatment, often in combination with specific anti-parasitic drug therapy. The choice of treatment must primarily be based on the ultrasound images of the cyst and also on the medical infrastructure and human resources available. For alveolar echinococcosis, early diagnosis and radical surgery followed by anti-infective prophylaxis with albendazole remain the key elements. If the lesion is confined, radical surgery can be curative. Unfortunately, the disease is diagnosed at an advanced stage in many patients. As a result, if palliative surgery is carried out without complete and effective anti-infective treatment, frequent relapses will occur.