

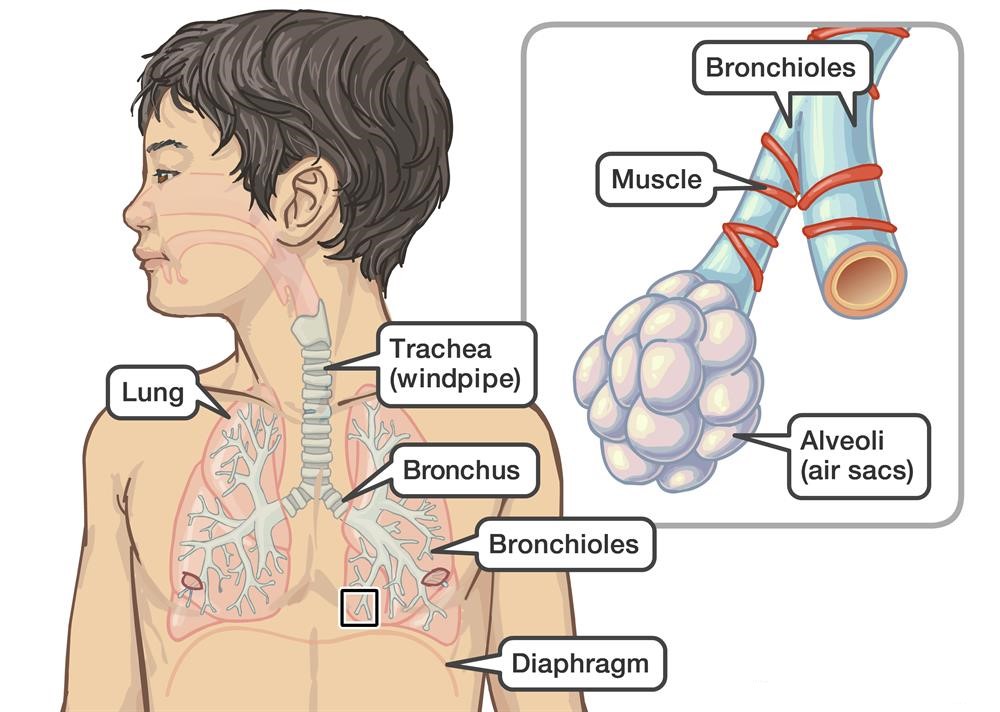
RSV is a very common virus that can lead to a viral respiratory tract infection that affects the lungs and respiratory tract in adults and older healthy children. It is a medium-sized (120-200 nm) enveloped virus that contains a lipoprotein coat and a linear negative-sense RNA genome. Human RSV can be divided into two antigenic subgroups, A and B, according to the reactivity of the virus with monoclonal antibodies against the attachment (G) and fusion (F) glycoproteins. RSV is transmitted through tiny droplets containing the virus when someone blows their nose, coughs, or sneezes. It also spreads through touching something that is contaminated by RSV.
Most people infected with RSV may have mild, cold-like symptoms:
However, some people, like premature babies, older adults, infants and adults with heart and lung disease, or anyone with a very weak immune system, are more likely to develop severe RSA infection and need to be hospitalized. These symptoms may include:
RSV is easily spread by touching infected people or surfaces having the virus on them. Therefore, good hygiene and keeping away from people who have fevers or colds are helpful to avoid and prevent RSV. There is currently no vaccine for RSV. But a drug called palivizumab may prevent RSV infection and protect high-risk baby from serious complications of RSV. If your doctor says your baby is at high risk (e.g. premature infants with chronic lung disease, and certain infants younger than 12 months old with congenital heart disease), she or he may recommend a monthly injection during the peak RSV season.
There is no medicine for the virus itself. Treatment regimens for RSV are to relieve the symptoms of infection. Most cases of RSV are mild and don't need medical treatment from doctors. Some careful at-home care is enough. While some severe cases of RSV may need treatment in a hospital where they can be watched closely and get fluids. Sometimes, doctors give medicine to help open airways.
The lipoprotein coat contains F, G, and SH lipoproteins. The F and G lipoproteins are the only two that target the cell membrane, and are highly conserved among RSV isolates. They serve as promising drug targets for RSV treatment.
F glycoprotein is a type I integral membrane protein that is highly conserved in RSV isolates of both subgroups A and B and has more than 90% identity in amino acid sequence. Due to the relatively conserved sequence, coupled with its role in viral entry, F glycoprotein is an ideal target for neutralizing antibodies. F protein has been examined as a vaccine antigen, and as the target of antibodies for passive prophylaxis.
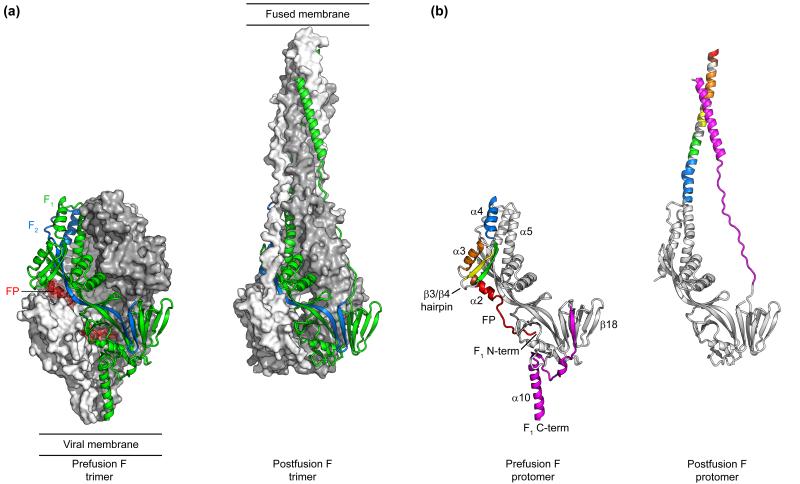 Fig.1 Conformations of the RSV F ectodomain (Mclellan. 2015).
Fig.1 Conformations of the RSV F ectodomain (Mclellan. 2015).
G glycoprotein is the major attachment protein of RSV. Its backbone contains 289 to 299 amino acids (32-33 kDa), depending on the strain, and is palmitoylated. It has no sequence homology with other paramyxovirus attachment proteins, and no hemagglutinating or neuraminidase functions. G glycoprotein plays an essential role in host cell attachment and modulation of host immunity. It has been revealed that G glycoprotein has a CX3C chemokine motif that can bind CX3CR1 and regulate CXCL1-mediated responses. And G glycoprotein and the G protein CX3C motif decrease the antiviral T cell response to RSV infection. Besides, the central region of the G protein contains a highly conserved 13-amino acid domain, partially overlapping the cysteine noose domain with 4 cysteines connected by 1-4 and 2-3, followed by a highly basic heparin-binding domain (HBD). HBD is a possible attachment site to heparan sulfate (HS) found on the surface of most cells. A peptide from the G protein HBD can efficiently bind to HEp-2 cells and inhibit RSV infection.
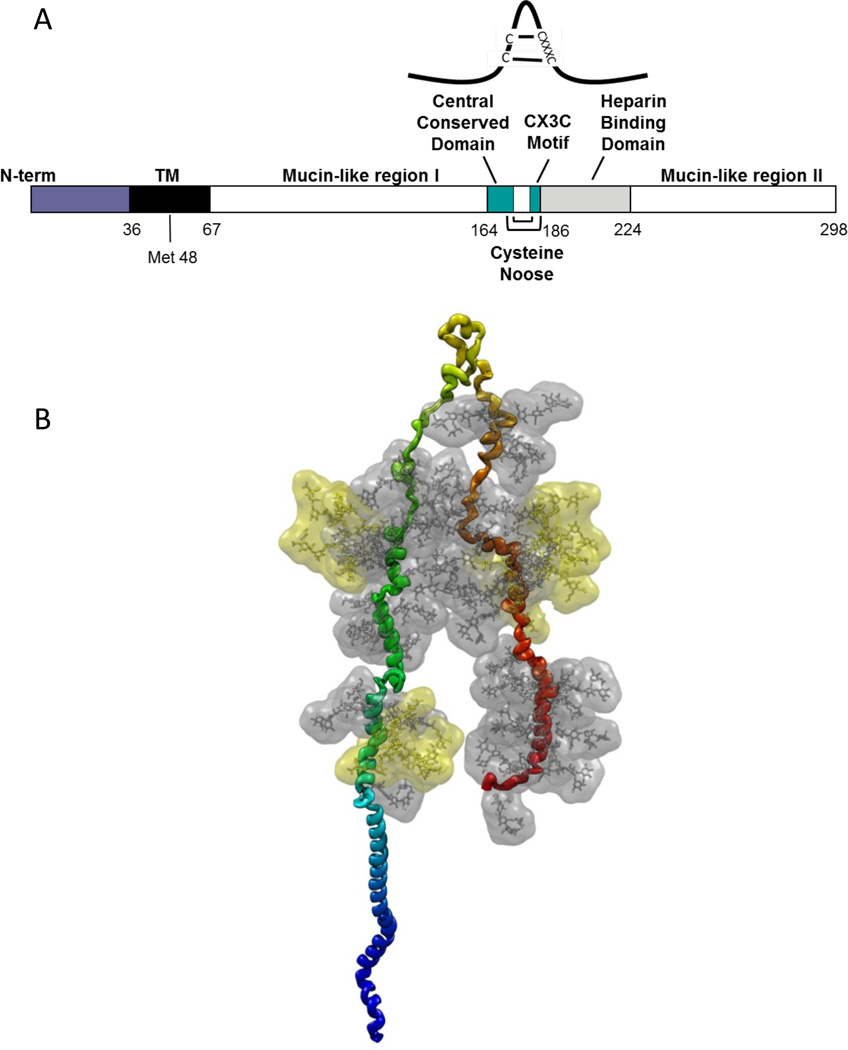 Fig 2. Schematic of the RSV G protein (Mclellan et al. 2013).
Fig 2. Schematic of the RSV G protein (Mclellan et al. 2013).
References: