Backgrounds
Bartter syndrome comprises a set of autosomal recessively inherited renal tubular disorders and is characterized by hypokalemic alkalosis, sodium and potassium wasting, hyperreninism, hyperaldosteronism, increased levels of angiotensin without hypertension and edema, and hyperplasia of the renal juxtaglomerular apparatus. Additional clinical and biochemical features lead to a classification into three phenotypical tubulopathies: (1) Gitelman syndrome (or hypocalciuria hypomagnesemia syndrome), (2) antenatal Bartter syndrome (or hyperprostaglandin E syndrome) and (3) classic Bartter syndrome (or Bartter syndrome type 3). Bartter syndrome is usually diagnosed in infancy or childhood, and all forms of this malady can capture symptoms of hypokalemia, metabolic alkalosis, and secondary hyperaldosteronism.
Characteristics of Bartter Syndrome
There are several characteristics used to distinguish each syndrome. In Bartter syndrome, the defect resides is at the thick ascending limb (TAL) of the loop of Henle, while the site of defect in Gitelman syndrome, at the distal convoluted tubule (DCT). As for patients with Bartter syndrome in early childhood, the failure to thrive is more serious and may cause a great deal of growth retardation. And Gitelman syndrome present is associated with less risk to grow and milder growth retardation. Gitelman symptom is similar to thiazide diuretic-abusers with salt wasting. Both of two symptoms show some common complaints with constipation, muscle cramps and weakness, secondary to chronic hypokalemia, along with non-specific dizziness and fatigue. Patients with either syndrome can be aggravated by diarrhea or vomiting into life-threatening rhabdomyolysis, cardiac arrhythmia, and syncope.
Pathogenesis of the Bartter Syndromes
The gene defect Bartter syndrome Type 1 occurs on chromosome band 15q21.1, as well as Type 2 and Type 4, is previously grouped into antenatal Bartter syndrome. Patients with Type 1 are due to the gene mutation for Na-K-Cl cotransporter (NKCC2) and on the apical membrane of LOH. As for Bartter syndrome Type 3, it is what referred to classic Bartter syndrome. Type 1, 2 and 4 Bartter syndrome present at a younger age than classic Type 3. Their patients with symptoms are often quite severe in the neonatal period. Classic Bartter syndrome Type 3 appears later in life and maybe mildly symptomatic or sporadically asymptomatic. And Type 5 attributed to calcium sensing receptor (CASR) mutation gives rise to a condition marked by hypocalcemia, suppressed parathyroid hormone function with the Bartter-like syndrome. There are numerous hypotheses regarding the underlying pathogenesis of the Bartter syndromes proposed, including:
- Primary juxtaglomerular hyperplasia
- Primary insensitivity to angiotensin II
- Primary prostaglandin-kallikrein-kinin overproduction
- Primary defects in NaCl transport in various nephron segments
- Primary defect in K transport resulting in excessive K excretion
- And (f) primary defect in Cl transport in the thick ascending limb (TAL) of Henle's loop or the distal convoluted tubule (DCT)
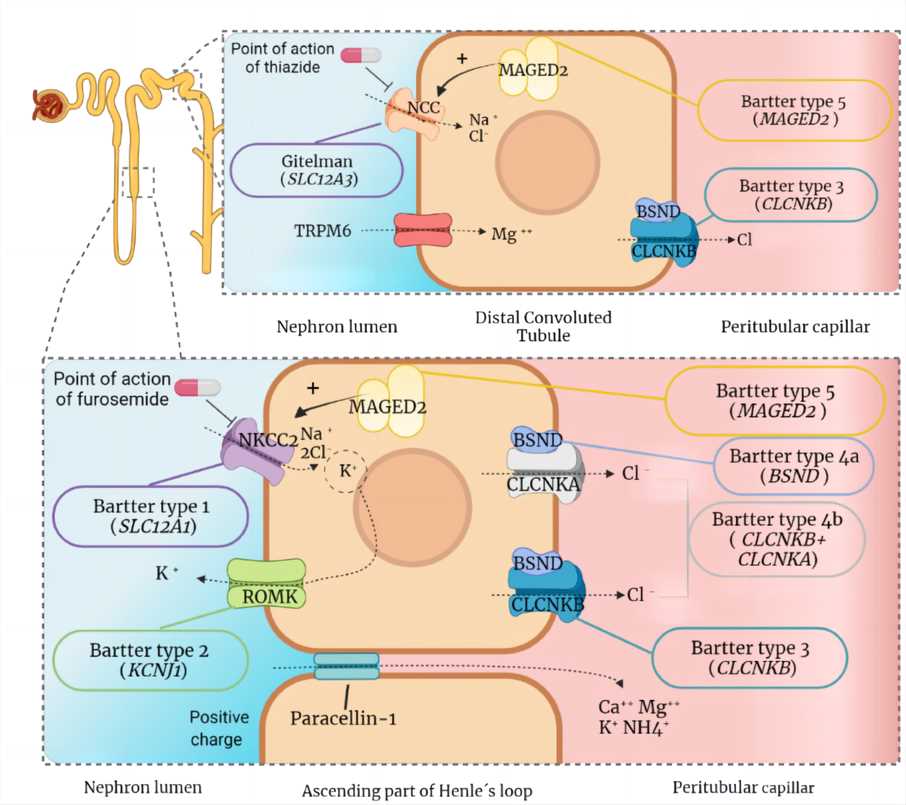 Fig.1 Implicated proteins and channels in the pathogenesis of Gitelman and Bartter syndromes.1
Fig.1 Implicated proteins and channels in the pathogenesis of Gitelman and Bartter syndromes.1
Diagnosis and Treatments
There was a report that one patient's renal biopsy was performed on the 17th postpartum day and hyperplasia of the renal juxtaglomerular apparatus was visible by light microscopy. This pathological discovery confirmed the diagnosis of Bartter syndrome. Despite more advance in elucidating the pathogenesis of Bartter syndromes, therapies aimed to correct the primary defects are not yet available. Thus, the main remedial objective is to improve the hypokalemic, hypochloremic and metabolic alkalosis. Patients should be encouraged to ingest liberal amounts of sodium and potassium in their diet, potassium supplements (e.g. potassium chloride) are usually used, and spironolactone is also chosen to reduce potassium loss. Furthermore, nonsteroidal anti-inflammatory drugs (NSAIDs) can be utilized and positively helpful in patients with neonatal Bartter syndrome. Angiotensin-converting enzyme (ACE) inhibitors have effects on this syndrome as well.
Creative Biolabs works as one of the most experienced specialists in antibody development, particularly in the in vitro diagnostic (IVD) antibody discovery. We offer customized IVD antibody development services targeting different biomarkers of Bartter syndrome type 1 to obtain high-quality antibodies for immunoassay development. Besides, we also offer diagnostic immunoassay development services, including feasibility analysis, assay design, assay protocol establishment, assay optimization, and kit production.
Our IVD antibody development services target different biomarkers of Bartter Syndrome Type 1, including but not limited to:
Reference
- Nuñez-Gonzalez, Laura, Noa Carrera, and Miguel A. Garcia-Gonzalez. "Molecular basis, diagnostic challenges and therapeutic approaches of bartter and gitelman syndromes: a primer for clinicians." International Journal of Molecular Sciences 22.21 (2021): 11414. Distributed under Open Access license CC BY 4.0, without modification.
For Research Use Only.