Hypoxic in Renal Disease
The oxygen of kidney is maintained at comparatively stable levels and its availability is determined by the complex interactions among a lot of biological processes, such as oxygen consumption, arterial-to-venous oxygen shunting, renal blood flow, glomerular filtration, medullary architecture, and Na+ transport. When this delicate balance is disrupted, the renal tissue may be susceptible to hypoxic injury. Indeed, a theory that renal hypoxia is implicated as one of the major causes of acute kidney injury (AKI) and chronic kidney diseases (CDK) has been validated by numerous studies. Recently, renal hypoxia is emerging as a key role in the pathology and physiology of the AKI-to-CKD transition. Factors possibly contributing to renal hypoxia in chronic kidney disease:
- Anemia
- Renal artery stenosis
- Loss of peritubular capillaries
- Impaired peritubular blood flow due to glomerular hypoperfusion and/or an imbalance of vasoactive substances
- Increased diffusion barriers due to tubulointerstitial fibrosis.
Some regions of the kidney are physiologically considered hypoxic despite reaching up to 20 percent of the cardiac outputs in human beings. According to reports, the partial pressure of oxygen in renal cortex in normal animals is between 20 to 60 mmHg, while the corticomedullary junction and medulla are exposed to prominent hypoxia, approximately 10-30 mmHg. Here, one critical reason of renal hypoxia, especially in the medulla, is the arterial-to-venous oxygen shunt. Another cause is that the kidney is required to reabsorb quantities of solutes (mostly Na+) and water, which needs mitochondrial respiration and ATP production at high standards. On the basis of these characteristics, there was an opinion proposed that hypoxia in the tubulointerstitium of injured kidneys is the final common pathway that leads to the end-stage kidney disease (ESKD). Additionally, the main cause of ESRD is CKD and a host of methods have exhibited aggravated renal hypoxia in animal models of CKD. All the risk factors associated with CKD produce inappropriately low oxygen tensions within the kidney. There appears to be a direct link between hypoxia and the progression of CKD.
Hypoxia-inducible Factor
CKD as the worldwide disease burden has become an urgent issue; however, new therapeutic options for it are still limited. Renal hypoxia takes an important position in the process of AKI and CKD. It is now accepted broadly that the activation of hypoxia-inducible factor (HIF), which is a pivotal transcription factor in cellular adaptation to hypoxia, protects the kidney during AKI. But the protective role of chronic HIF activation in CKD remains controversial at some extent.
HIF is a major mediator in tissue and cellular adaptation to hypoxia. It upregulates the transcription of more than 100 target genes controlling hematopoiesis, angiogenesis, and anaerobic metabolism. HIF is a heterodimeric transcription factor consisting of alpha (HIF-α) and beta (HIF-β) subunits. Under normoxic circumstances, HIF-1α takes unique post-translational modification by factor inhibiting HIF-1 (FIH-1), that is an asparaginyl hydroxylase modifying one specific asparagine residue of HIF-1α. This modification inhibits the binding of coactivators CBP (CREB-binding protein) and p300, leading to repressed transactivation. FIH-1 is largely expressed in distal tubules and podocytes, and it reveals a lower Km value for oxygen than PHD. Thereby, HIF-1α is stabilized by escaping degradation through the PHD/pVHL pathway and still experiences FIH-1-mediated oxygen-dependent transactivational regulation in a certain range of oxygen tension.
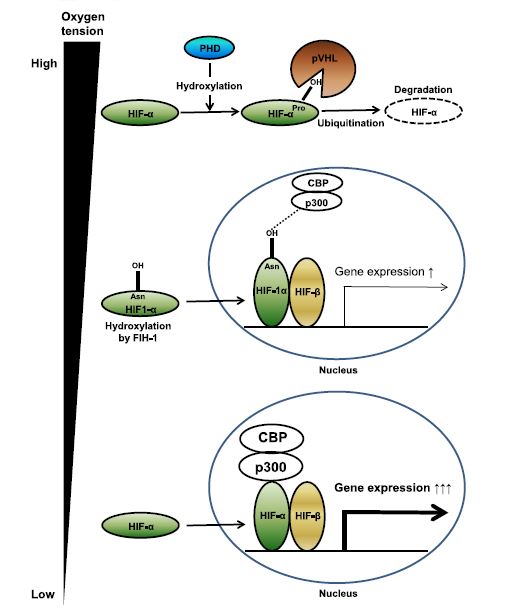 Fig.1 HIF genes and regulations.1
Fig.1 HIF genes and regulations.1
Role of Hypoxia in the Renal Disease
The kidney shows a noticeable discrepancy between blood supply and oxygenation. In spite of high blood flow and oxygen delivery, oxygen tensions in the kidney are relatively low, particularly in the renal medulla. The reason for that lies in the parallel arrangement of arterial and venous, preglomerular and postglomerular vessels, which permits oxygen to pass from arterioles into the postcapillary venous via shunt diffusion. The limitation of renal oxygen supply depicts the kidney susceptible to hypoxia and has been recognized as an important factor in the pathogenesis of AKI.
As a leader in the advancing antibody market, Creative Biolabs provides custom IVD antibody development and production services to scientists around the world to support and accelerate their IVD projects. The services we provide include antibody generation, antibody conjugation, and immunoassay development. Our services are fully customized against different targets of different human diseases, including renal hypoxia.
Our IVD antibody development services target the following biomarkers of renal hypoxia:
Reference
- Tanaka, Shinji, Tetsuhiro Tanaka, and Masaomi Nangaku. "Hypoxia and hypoxia-inducible factors in chronic kidney disease." Renal Replacement Therapy 2 (2016): 1-8. Distributed under Open Access license CC BY 4.0, without modification.
For Research Use Only.