With the global pandemic of coronavirus disease 2019 (COVID-19) caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) still ongoing, the prevention and treatment of COVID-19 has become a research focus in academia and pharmaceutical industry. In addition to the research and development of SARS-CoV-2 neutralizing antibodies, extensive clinical data have demonstrated the over-activation of the complement system in COVID-19 patients, which induces cytokine storms and acute respiratory distress syndrome (ARDS), or more severely, multi-organ failure. Since over-activation of the complement system is the trigger for a series of subsequent symptoms of COVID-19, is it possible to intervene the complement system and develop new therapeutic strategies?
In July 2020, an article entitled “Association of COVID-19 inflammation with activation of the C5a-C5aR1 axis” published on Nature revealed the association of COVID-19 and activation of the C5a-C5AR1 axis. Studies have shown that restraining the activity of complement system by inhibiting C5a-C5AR1 can help to restore normal function of immune system against virus infection. To this end, scientists have done a lot of research on the effector molecules in the complement system, and a number of C5AR1-targeted drugs are in the clinical stage.
Introduction to C5AR1
C5AR1 (C5a anaphylatoxin chemotactic receptor 1, C5a-R or CD88) is a classical G protein-coupled receptor. C5AR1, also known as the complement activation fragment C5a receptor, plays a key role in the innate immune response. As part of the complement system, the complement C5a binds to its receptor C5AR1, activating the C5AR1-C5a axis. C5AR1 interacts with C5a to exert pro-inflammatory effects. C5AR1 is mainly expressed on granulocytes, monocytes, dendritic cells, and MDSCs (myeloid-derived suppressor cells) in various tumor tissues. Numerous studies have shown that a variety of related diseases, including chronic kidney disease, cardiovascular disease, neurological disease, and cancer, can be treated by targeting C5AR1-C5a axis. What’s more, a study reported in Nature confirmed that severe COVID-19 symptom is associated with a systemic inflammatory response, with inflammation and blood clotting in the patient’s body, accompanied by lung and kidney damage, which provides important biomarkers and potential treatments for COVID-19.
The Mechanism of C5AR1-C5a in COVID-19
In the human body, C5AR1 binds to C5a to trigger an inflammatory signal. Abnormal complement activation leads to excessive C5AR1-C5a signaling, which is responsible for many autoinflammatory diseases. In critically ill patients with COVID-19, scientists have found that after the activation of the complement C5AR1-C5aR axis, pulmonary neutrophils and monocytes can be recruited and activated to participate in ARDS. The study pointed out that the increase of soluble C5a was proportional to the severity of COVID-19; meanwhile, the expression of C5AR1 in myeloid-derived cells in peripheral blood and lung was increased, suggesting that the C5AR1-C5aR axis may be involved in the development of ARDS.
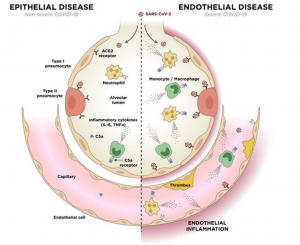
(Julien Carvelli et al., Nature, 2020)
On October 8, 2021, ChemoCentryx’s first drug targeting C5AR1 (Avacopan) was launched for the treatment of neutrophil cytoplasmic autoantibody-associated vasculitis and granuloma. In terms of COVID-19 treatment, C5AR1 drug development is challenging, and has not yet translated into clinical benefit, but it is worth looking forward to.
Complement drugs have received much attention in pharmaceutical industry in recent years. After ChemoCentryx’s C5AR1 small molecule inhibitor was approved by the FDA, ChemoCentryx’s share price also doubled to a market value of $2.7 billion. At present, the four targets C5a, C3, C5 and C5AR1 in the complement system have all been carried out for related research on COVID-19.