- Home
- Resources
- Featured Solutions
- One-Stop ADC Development Solution
- ADC In Vitro Analysis Solution
- ADC In Vivo Analysis Solution
- ADC In Vivo Efficacy Evaluation: CDX, PDX & Syngeneic Models
- ADC Solid Tumor Model Evaluation: Preclinical Efficacy & TK Studies
ADC Solid Tumor Model Evaluation: Preclinical Efficacy & TK Studies
Translating antibody-drug conjugate (ADC) candidates from the bench into credible in vivo efficacy datasets demands tumor models that reflect the biological complexity of human disease. Creative Biolabs provides a comprehensive xenograft-based evaluation platform that integrates subcutaneous, orthotopic, and bioluminescent imaging models with multi-endpoint pharmacodynamic readouts. Supported by an extensive cell line repository spanning 10 solid tumor types and a team experienced in both surgical orthotopic implantation and non-invasive longitudinal monitoring, we deliver efficacy data that helps research teams prioritize lead candidates with confidence during the pre-clinical discovery phase.
Inquire for Pre-clinical SupportOverview: Xenograft Models as the Workhorse of ADC Efficacy Testing
Cell line-derived xenograft (CDX) models represent the most widely adopted platform for evaluating the antitumor activity of antibody-drug conjugates in solid tumor research. By implanting well-characterized human cancer cell lines into immunodeficient mice, researchers can generate reproducible tumor growth kinetics and interrogate the relationship between target antigen expression, payload mechanism, and tumor response under controlled conditions.
Two Complementary Implantation Strategies
Xenograft models for ADC evaluation fall into two broad categories, each serving a distinct purpose in the efficacy assessment workflow:
- • Heterotopic (Subcutaneous) Xenografts: Cancer cells are injected into the flank or dorsal region of immunodeficient mice. Tumors develop in a readily accessible location, allowing direct caliper measurement of volume and convenient dosing. Subcutaneous models are the standard first-line approach for establishing dose-response relationships, defining tumor growth inhibition (TGI) values, and screening multiple ADC candidates in parallel.
- • Orthotopic Xenografts: Tumor cells or tissue fragments are surgically implanted into the organ of origin (e.g., mammary fat pad for breast cancer, pancreas for pancreatic cancer). These models recapitulate the native tissue microenvironment including organ-specific stromal interactions, vascular architecture, and metastatic potential. Orthotopic models are particularly valuable for ADCs targeting antigens whose expression is modulated by the tumor microenvironment.
Host Strain Selection for Xenograft Studies
| Mouse Strain | Immunodeficiency Level | Recommended Application |
|---|---|---|
| Nude (nu/nu) | T-cell deficient; intact NK cells and macrophages | Subcutaneous CDX models with standard cell line engraftment; cost-effective initial screening |
| SCID | T- and B-cell deficient; intact NK cells | Moderate engraftment of hematopoietic and solid tumor lines; suitable for ADC efficacy with low NK-mediated clearance |
| NSG / NOG | Severely immunodeficient (T, B, NK deficient) | High-engraftment orthotopic models; preferred for metastatic monitoring and bioluminescent imaging studies |
Key Challenges in ADC Efficacy Evaluation Using Solid Tumor Models
Designing a xenograft study that yields interpretable, translationally relevant ADC efficacy data is not straightforward. Several factors routinely compromise data quality or delay project timelines:
- ▶ Antigen Expression Mismatch: Cell lines used for CDX models may drift in target antigen expression over passages. An ADC that relies on a specific receptor density threshold may appear inactive in in vivo models simply because the implanted cells no longer express the target at clinically relevant levels.
- ▶ Limited Metastatic Readout: Standard subcutaneous models rarely metastasize, which means ADCs designed to target disseminated disease cannot be fully characterized. This gap can mask efficacy differences between linker-payload combinations that may only become apparent in a metastatic setting.
- ▶ Endpoint Selection Ambiguity: Relying solely on tumor volume measurements misses pharmacodynamic (PD) insights. An ADC may slow proliferation without shrinking tumors, which caliper-based TGI alone cannot distinguish from a genuinely cytotoxic response. Correlative biomarker analysis is essential but adds complexity to study planning.
- ▶ Orthotopic Model Accessibility: Tumors growing in deep organs (pancreas, lung, ovary) cannot be measured with calipers. Without non-invasive imaging, longitudinal tracking requires terminal cohorts at each time point, inflating animal numbers and cost while sacrificing temporal resolution.
Our Solid Tumor Model Solutions for ADC Evaluation
Creative Biolabs addresses these challenges through a modular platform that combines model diversity, analytical depth, and imaging integration into a cohesive efficacy evaluation package:
| Solution | What It Resolves | Supporting Capabilities |
|---|---|---|
|
Primary Model Subcutaneous CDX Models Standard flank-implantation models using validated, antigen-characterized human cancer cell lines across 10 solid tumor types. |
• Eliminates antigen drift risk through pre-implantation expression validation. • Enables head-to-head comparison of multiple ADC candidates under identical host conditions. • Supports standard TGI, tumor mass, and body weight change endpoints. |
• 70+ validated cell lines across pancreatic, breast, ovarian, melanoma, prostate, renal, colorectal, lung, mesothelioma, and multiple myeloma. • Nude, SCID, and NSG host strains matched to cell line engraftment characteristics. |
|
Microenvironment-Relevant Orthotopic Implantation Models Surgical implantation of tumor cells or tissue into the organ of origin, preserving tissue-specific stromal and vascular architecture. |
• Enables evaluation of ADC penetration into organ-specific extracellular matrix. • Supports spontaneous metastasis tracking for late-stage efficacy readouts. • Provides a more clinically relevant tumor microenvironment for microenvironment-sensitive payloads. |
• Experienced surgical team for mammary fat pad, pancreatic, intraperitoneal, and orthotopic lung implantation. • Post-operative care protocols minimizing surgical stress artifacts in efficacy data. |
|
Longitudinal Imaging Bioluminescent Xenograft Monitoring Firefly luciferase-transduced cell lines with D-luciferin-based bioluminescence imaging for non-invasive tumor burden tracking. |
• Overcomes the caliper-accessibility limitation of orthotopic models. • Enables early detection of tumor engraftment (signal detectable from ~1,000 cells). • Reduces animal numbers by replacing terminal time-point cohorts with longitudinal imaging. |
• Non-invasive imaging systems for whole-animal bioluminescence quantification. • Luciferase transduction service available for custom cell lines not yet in our luciferase library. |
|
Multi-Endpoint PD Integrated Pharmacodynamic Profiling Combination of terminal tumor analysis with protein, histological, and molecular readouts for a complete picture of ADC mechanism of action in vivo. |
• Distinguishes cytostatic from cytotoxic ADC activity via proliferation marker analysis. • Verifies target engagement through IHC confirmation of payload delivery to tumor tissue. • Correlates PK exposure data with PD response to anchor the efficacy interpretation. |
• ELISA & Western blotting for intracellular target modulation and apoptosis markers. • Immunohistochemistry & H&E staining for histological response grading. • RT-qPCR for transcriptional-level target and pathway analysis. |
Structured Workflow for Solid Tumor ADC Evaluation
Every efficacy study follows a standardized sequence that moves from model selection through data delivery, ensuring reproducibility and decision-ready results:
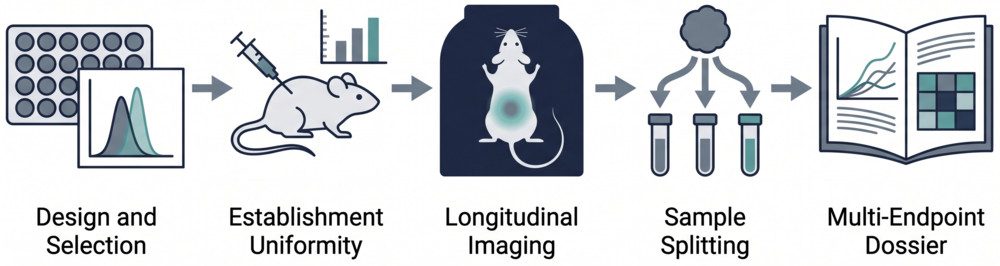
Phase 1: Study Design & Match-to-Model Selection
We review the ADC target antigen profile, payload mechanism, and research goals to select the appropriate cancer type, cell line, implantation method, and host strain. Target antigen expression on candidate cell lines is confirmed by flow cytometry or IHC before model initiation to ensure biological relevance.
Phase 2: Model Establishment & Quality Gate
Tumor cells are implanted via subcutaneous injection or surgical orthotopic implantation. For bioluminescent studies, luciferase-expressing lines are used. Engraftment is monitored, and animals are randomized into treatment groups once tumors reach a predefined volume range, ensuring uniform starting tumor burden across all cohorts.
Phase 3: Dosing & Longitudinal Monitoring
ADC candidates are administered according to the agreed dosing schedule. Standard measurements (body weight, tumor caliper volume) are recorded at each time point. For orthotopic or bioluminescent models, whole-animal imaging captures tumor burden at scheduled intervals, generating a continuous growth curve without terminal sampling.
Phase 4: Terminal Endpoint & Sample Collection
At study termination, tumors are excised, weighed, and processed for downstream analysis. Blood is collected for pharmacokinetic correlation if required. Tumor tissue is split for formalin fixation (histology), protein extraction (ELISA/Western blot), and RNA isolation (RT-qPCR), depending on the pre-specified PD panel.
Phase 5: Multi-Endpoint Analysis & Reporting
All data streams (tumor growth curves, TGI calculations, body weight trajectories, imaging quantification, and PD biomarker results) are integrated into a comprehensive efficacy report. Statistical comparisons between treatment and control groups are performed, and the final dataset is delivered with a detailed methods section suitable for inclusion in regulatory or publication documents.
Technology Platforms Supporting Solid Tumor ADC Evaluation
Our efficacy platform draws on a combination of animal facility infrastructure, cell line resources, imaging systems, and analytical instrumentation to deliver reliable, multidimensional datasets:
1. Rodent Facility & Surgical Suite
A barrier-maintained animal facility housing nude, SCID, and NSG mouse colonies under standardized husbandry conditions. The facility includes a dedicated surgical suite for orthotopic implantation, with post-operative recovery monitoring and aseptic technique protocols that minimize surgical stress as a confounding variable in efficacy studies.
- • Multiple immunodeficiency levels: Allows matching of host strain to cell line engraftment efficiency.
- • Controlled environment: Temperature, humidity, and light-cycle regulation to reduce inter-experiment variability.
- • Ethical compliance: All studies conducted under IACUC-equivalent oversight with humane endpoint criteria.
2. Characterized Cancer Cell Line Repository
A curated collection of over 70 human cancer cell lines across 10 solid tumor types. Each line is maintained with documented antigen expression profiles, doubling times, and in vivo growth characteristics. Lines are authenticated by short tandem repeat (STR) profiling and routinely screened for contamination, ensuring that efficacy data are built on a reliable biological substrate.
- • 10 cancer types covered: Pancreatic, breast, ovarian, melanoma, prostate, renal, mesothelioma, colorectal, lung, and multiple myeloma.
- • Target-annotated: Cell lines cross-referenced with common ADC targets (HER2, CD74, mesothelin, PSMA, FAP, nectin-4, and others).
- • Luciferase-ready sub-lines: Pre-transduced firefly luciferase-expressing variants for immediate bioluminescent imaging studies.
3. Non-Invasive Bioluminescence Imaging System
A whole-animal optical imaging platform capable of detecting and quantifying firefly luciferase bioluminescence following D-luciferin substrate injection. The system enables longitudinal tracking of orthotopic and metastatic tumor burden without requiring terminal procedures, supporting both primary tumor and metastatic dissemination endpoints within the same animal.
- • Detection sensitivity: Signal detectable from approximately 1,000 luciferase-expressing cells in vivo.
- • Longitudinal capability: Repeated imaging across weeks without animal sacrifice, preserving temporal resolution.
- • Quantitative output: Region-of-interest photon flux values for statistical comparison between treatment groups.
4. Histopathology & Molecular Analysis Laboratory
A fully equipped laboratory for terminal tumor analysis, providing the histological and molecular confirmation needed to move beyond volume-based endpoints. Standard services include tissue processing, paraffin embedding, sectioning, H&E staining, and immunohistochemistry, alongside protein and nucleic acid extraction for biochemical and transcriptional profiling.
- • IHC panel: Proliferation (Ki-67), apoptosis (cleaved caspase-3), target antigen, and payload distribution markers.
- • Protein analysis: ELISA and Western blotting for intracellular signaling and apoptosis pathway readouts.
- • Gene expression: RT-qPCR for target gene, drug resistance marker, and tumor microenvironment gene panels.
Why Choose Our Solid Tumor Efficacy Evaluation Services?
Model Diversity Matched to Research Question
We do not default to a single model type. Whether your ADC program needs rapid TGI screening in subcutaneous CDX, microenvironment-sensitive orthotopic evaluation, or non-invasive longitudinal monitoring via bioluminescence, the model is chosen to answer your specific question rather than conform to a one-size-fits-all protocol.
Multi-Endpoint Integration
Efficacy is not measured by tumor volume alone. Our standard workflow integrates body weight change, tumor mass, histological response grading, and optional PD biomarker panels, providing a three-dimensional view of ADC activity that informs both candidate ranking and mechanism-of-action understanding.
Antigen-Verified Starting Material
Every cell line used in an efficacy study undergoes target antigen expression verification by flow cytometry or immunohistochemistry before implantation. This quality gate prevents the common pitfall of testing an ADC in a model that no longer expresses the intended target, saving time and resources at the project level.
Seamless Connection to Downstream Analysis
Efficacy data generated in our solid tumor models feed directly into our pharmacokinetic characterization, safety assessment, and immunogenicity analysis services. This integration allows research teams to build a unified preclinical data package for a single ADC candidate without managing multiple vendor handoffs.
Research Insights: Advancing Solid Tumor Models for ADC Evaluation
According to Marques da Costa et al., orthotopic bioluminescent xenograft models combining luciferase-transduced cell lines with non-invasive imaging provide a powerful platform for tracking primary tumor growth and metastatic dissemination without terminal time-point cohorts. Their work demonstrated that bioluminescent signal from as few as 1,000 cells can be reliably detected in vivo, enabling treatment response monitoring at a resolution unattainable with caliper measurements alone.
Key Advances in Preclinical Tumor Modeling:
- • Orthotopic implantation: Tumor cells implanted in the organ of origin retain organ-specific stromal interactions and gene expression profiles, making these models superior for evaluating ADCs whose target antigen or payload activity is modulated by the tissue microenvironment.
- • PDX fidelity: Patient-derived xenograft models preserve the genomic heterogeneity of the original tumor across passages, enabling efficacy evaluation against clinically relevant mutational backgrounds that cell line-based systems cannot replicate.
- • ADC dosing translation: Recent work by Rubahamya demonstrated that approved ADCs achieve substantial efficacy in mouse models at weight-based doses comparable to clinical regimens, validating the translational relevance of well-designed xenograft studies for predicting human therapeutic windows.
Collectively, these advances underscore the importance of selecting the right model for the right question — a principle that guides every efficacy study at our facility.
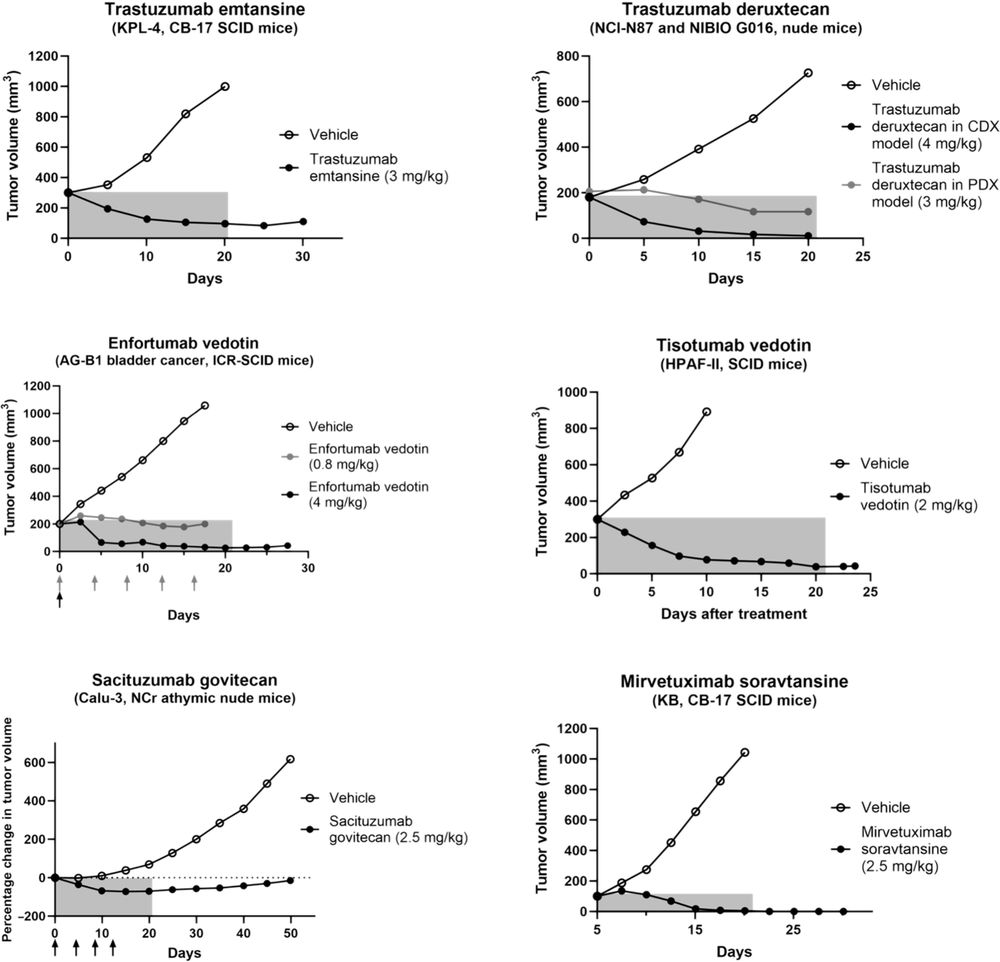
Fig.1 Preclinical efficacy of FDA-approved ADCs against solid tumors in mouse models.3,5
FAQs about ADC Solid Tumor Model Evaluation
Q: Which solid tumor types can you support for ADC efficacy evaluation?
A: We maintain characterized cell lines for 10 solid tumor types: pancreatic cancer, breast cancer, ovarian cancer, melanoma, prostate cancer, renal cancer, mesothelioma, colorectal cancer, lung cancer, and multiple myeloma. For each cancer type, multiple cell lines with documented target antigen expression profiles are available, allowing researchers to select models that match their ADC's specificity for pre-clinical in vivo testing.
Q: How do I decide between a subcutaneous and an orthotopic model for my ADC candidate?
A: Subcutaneous models are the standard starting point for dose-response and TGI studies due to their reproducibility, ease of measurement, and lower cost. Orthotopic models are recommended when your ADC's target antigen is known to be regulated by the tissue microenvironment, when you need to evaluate metastatic dissemination, or when your payload mechanism (e.g., an anti-stromal or hypoxia-activated warhead) requires organ-specific context for full activity. We can help you assess which approach aligns with your program stage and research goals during study design.
Q: What endpoints are included in a standard solid tumor efficacy study?
A: A standard study includes body weight change monitoring, food consumption tracking, tumor volume growth curves (by caliper for subcutaneous models or bioluminescent imaging for orthotopic models), terminal tumor mass, and tumor growth inhibition (TGI) calculation. Additional PD biomarker analyses (ELISA, Western blot, IHC, H&E, RT-qPCR) can be added to the scope depending on your research objectives, providing a more detailed picture of ADC mechanism of action in vivo.
Q: Can you accommodate custom cell lines or luciferase transduction for our specific ADC target?
A: Yes. While our repository includes over 70 pre-characterized cell lines, we routinely work with client-provided cell lines. We can perform luciferase transduction on your cell line of choice to enable bioluminescent imaging, and we verify target antigen expression before model initiation regardless of whether the cell line comes from our repository or yours. This flexibility ensures the efficacy data are generated in the most biologically relevant system for your ADC candidate.
Q: How are bioluminescent imaging data quantified and reported?
A: Bioluminescence data are acquired as photon flux (photons per second) within a defined region of interest drawn over the tumor site. For each animal, measurements are taken at scheduled intervals throughout the study, generating a longitudinal bioluminescence growth curve analogous to a caliper-based tumor volume curve. The final report includes individual animal photon flux values, group mean curves with standard error, and statistical comparisons between treatment and control groups at each imaging time point, alongside correlative terminal tumor mass data when applicable.
Related Products
Related Resources

References:
1. Marques da Costa, Maria Eugenia, et al. "Establishment and characterization of in vivo orthotopic bioluminescent xenograft models from human osteosarcoma cell lines in Swiss nude and NSG mice." Cancer medicine 7.3 (2018): 665-676. https://doi.org/10.1002/cam4.1346.
2. Liu, Yihan, et al. "Patient-derived xenograft models in cancer therapy: technologies and applications." Signal Transduction and Targeted Therapy 8 (2023): 160. https://doi.org/10.1038/s41392-023-01419-2.
3. Rubahamya, Baron, Shujun Dong, and Greg M. Thurber. "Clinical translation of antibody drug conjugate dosing in solid tumors from preclinical mouse data." Science Advances 10.22 (2024): eadk1894. https://doi.org/10.1126/sciadv.adk1894.
4. Takakura, Toshiaki, Toshio Shimizu, and Nobuyuki Yamamoto. "Antibody-drug conjugates in solid tumors; new strategy for cancer therapy." Japanese Journal of Clinical Oncology 54.8 (2024): 817–826. https://doi.org/10.1093/jjco/hyae054.
5. Distributed under Open Access License CC BY 4.0, without modification.
For Research Use Only. NOT FOR CLINICAL USE.
Online Inquiry
Welcome! For price inquiries, please feel free to contact us through the form on the left side. We will get back to you as soon as possible.
