Creative Biolabs has a tradition of commitment. To achieve efficient execution and regulatory approval, we offer careful considerations of your program for the development of a cellular or gene therapy product – now and in the future.
EXPLORE MORE HighlightsWe focus on unmet needs and develop novel cellular and gene drugs and solutions that offer significant benefits over existing options.
EXPLORE MORE HighlightsThe advent of Chimeric Antigen Receptor T-cell (CAR-T) therapies has revolutionized the field of oncology, providing new avenues for treating various forms of cancer. Our 20 years of experience in the biotechnology sector have equipped us with the expertise and technological capabilities to support the entire lifecycle of CAR-T products, from early development to commercialization.
EXPLORE MORETo accelerate advanced breakthroughs of your projects, we offer broad range of platforms which enable our clients be free to tackle problems with cutting-edge technologies from different angles and in different methods.
EXPLORE MORE HighlightsUse the resources in our library to help you understand your options and make critical decisions for your study. We offer oncolytic virus, CAR-T, and dendritic cell related documents, as well as newsletter. If you don't find the answers you're looking for, contact us for additional assistance.
EXPLORE MORE HighlightsGet a real taste and understanding of the business and culture of one of the world's great research-based cellular and gene therapy discovery and development companies.
EXPLORE MORE
The Antibody-Coupled T-Cell Receptor (ACTR) platform is an autologous engineered T-cell therapy designed to combine with tumor-targeting antibodies to exert a powerful anti-tumor immune response and kill tumor cells. ACTR consists of an extracellular domain, a transmembrane domain, a co-stimulatory signaling domain, and a T cell receptor (TCR)signaling domain similar to Chimeric Antigen Receptor (CAR) design. The ACTR construct is derived from human CD16 and binds to the T cell signaling domain, and is designed to bind to the Fc domain of a therapeutic antibody, thereby providing a new platform for T cell-targeted cancer therapy. In contrast to CAR-T cell constructs that express the antigen targeting single chain variable fragment (scFv), ACTR T cell activity is regulated through antibody administration and is therefore not susceptible to target-mediated autolysis during T cell production. Thus, the ACTR platform is highly adaptable and can target multiple tumor antigens, thereby avoiding the need to generate and characterize multiple CAR-T therapies.
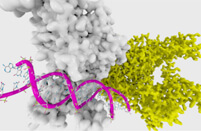
The TCR is a protein complex found on the surface of T cells or T lymphocytes, responsible for recognizing fragments of antigens as peptides bound to major histocompatibility complex (MHC) molecules. Structurally speaking, the TCR is formed by six different polypeptides. In most T cells, TCRs are composed of αβ subunits displaying immunoglobulin-like variable domains responsible for recognizing peptide antigens associated with MHC molecules expressed on the surface of antigen-presenting cells. TCRαβ subunits are associated with the CD3 complex formed by the γ, δ, ε and ζ subunits, which are invariant and ensure signal transduction. The binding between TCRs and antigenic peptides has relatively low affinity and is degenerate. In other words, many TCRs recognize the same antigenic peptide, and many antigen peptides are recognized by the same TCR. The ACTR construct is composed of the ectodomain of CD16 fused to intracellular co-stimulatory and CD3ζ signaling domains, which allow ACTR T cells to exert antibody-dependent cell-mediated cytotoxicity, a function otherwise physiologically limited to CD16-expressing natural killer cells and macrophages.
In ACTR, the antibody part of the cell attaches to a mAb delivered separately to the patient. First, the mAb locks onto the cancer cell and then ACTR locks onto the mAb. There are two key advantages of ACTR T cell therapy. First, the same ACTR cell type can be used against different cancers, so physicians only need to change the mAb biologic used in conjunction with ACTR. Second, when the patient stops taking the mAb, the adverse effects may cease, because discontinuing the mAb essentially acts as an "off" switch in cases where the immune response is too strong. The combination of ACTR and mAb could improve the safety of T cell therapy. Plus, mass producing the ACTR could reduce costs.
The ACTR platform has been developed to combine the anticancer potential of T cell and antibody therapies. On the one hand, T lymphocytes can exert major antitumor effects in cancer immunotherapy, as evidenced by the results of allogeneic hematopoietic stem cell transplantation in the treatment of hematological malignancies, in which T cell-mediated graft-versus-host disease is inversely associated with disease recurrence, and immunosuppression withdrawal or infusion of donor lymphocytes can contain relapse. The expression of chimeric signaling receptors with antibody recognition properties can skew the reactivity of T lymphocytes towards cancer cells: ligation of the cognate target results in T-cell activation and triggers cytotoxicity. On the other hand, administration of monoclonal antibodies (mAbs) can exert cytotoxicity through a variety of mechanisms, including induction of proapoptotic signals, complement fixation, and antibody-dependent cell cytotoxicity (ADCC). A major role is played by the mechanism of ADCC, which results from the engagement of Fc receptors (FcγR) expressed on the surface of natural killer (NK) cells and other cells, such as neutrophils and macrophages, by the Fc portion of the antibody. Polymorphisms of FcγR genes can have marked functional consequences, which, in turn, influence response to antibody treatment. Mechanistically speaking, although ACTR T cells cannot directly recognize tumor cells, once a tumor-targeting antibody is provided to bind to the surface of tumor cells, they can indirectly recognize tumor cells through the Fc domain of the antibody. This will enable ADCC to kill tumor cells. That is, ACTR T cells function by binding the Fc domain of a therapeutic antibody opsonized on target cells, resulting in T cell activation and tumor cell killing.
Autologous T cells engineered to express the universal ACTR chimeric receptor kill tumors through interactions with tumor-targeting antibodies. There are two ACTR constructs, ACTR087 and ACTR707, currently in clinical testing. ACTR087 and ACTR707 are being combined with rituximab in subjects with CD20+ B-cell lymphoma in two separate trials (NCT02776813 and NCT03189836, respectively).
ACTR087 expresses a 4-1BB-containing receptor and has been evaluated in combination with rituximab in subjects with relapsed or refractory (R/R) CD20+ B cell lymphoma. Preclinical findings with ACTR+ T cells, which bind immunoglobulin Fc via CD16V158 and signal via CD3ζ and 4-1BB (ACTR087), demonstrate markedly enhanced target- and antibody-specific tumor cell cytotoxicity, as evidenced by CD20+ B cell lymphoma killing in combination with rituximab, compared with rituximab alone. Preclinical data also demonstrate rituximab dose-dependent effects in combination with ACTR087, suggesting that the therapeutic index of ACTR087 in combination with rituximab may be affected by rituximab dose or schedule and present an advantage over CAR T cell therapies. ACTR087 is also being used in multiple myeloma subjects in combination with a novel BCMA-targeting antibody (NCT03266692).
ACTR707 comprises the extracellular domain of CD16 linked to a CD3ζ signaling domain and a CD28 co-stimulatory domain. ACTR707 is in clinical development in combination with rituximab (NCT03189836) or trastuzumab (NCT03680560). There are preliminary clinical results of a phase 1 study evaluating the safety and anti-tumor activity of ACTR707 in combination with rituximab in subjects with relapsed or refractory CD20+ B-cell lymphoma. ACTR707 in combination with rituximab induced complete responses in 3 of 6 subjects with relapsed or refractory aggressive CD20+ B cell lymphoma treated at the first dose level with ACTR707 in combination with rituximab, with no cytokine release syndrome (CRS), serious or severe (≥Gr3) neurotoxicity, or autoimmune adverse events (AEs) leading to treatment discontinuation. ACTR+ T cells were detectable in all subjects and persisted. These results support the continued dose escalation of ACTR707 in combination with rituximab. There are also preliminary clinical results from a phase 1 study of ACTR707 in combination with rituximab in subjects with relapsed or refractory CD20+ non-Hodgkin lymphoma. Data suggest that clinical responses can be achieved without severe T cell-mediated toxicities (eg, CRS and neurotoxicity) that have been reported with other autologous T-cell products.
Overall, in contrast to CAR T-cell constructs that are restricted to a single antigen, the ACTR platform is highly adaptable, and can be targeted against a diverse set of tumor antigens-thus circumventing the need to generate and characterize multiple CAR-T therapeutics. Although currently ACTR-expressing T cells have shown good cancer treatment effects in phase I clinical trials, more data are still needed to further confirm their efficacy and safety.
References
For any technical issues or product/service related questions, please leave your information below. Our team will contact you soon.
All products and services are For Research Use Only and CANNOT be used in the treatment or diagnosis of disease.
 NEWSLETTER
NEWSLETTER
The latest newsletter to introduce the latest breaking information, our site updates, field and other scientific news, important events, and insights from industry leaders
LEARN MORE NEWSLETTER NEW SOLUTION
NEW SOLUTION
CellRapeutics™ In Vivo Cell Engineering: One-stop in vivo T/B/NK cell and macrophage engineering services covering vectors construction to function verification.
LEARN MORE SOLUTION NOVEL TECHNOLOGY
NOVEL TECHNOLOGY
Silence™ CAR-T Cell: A novel platform to enhance CAR-T cell immunotherapy by combining RNAi technology to suppress genes that may impede CAR functionality.
LEARN MORE NOVEL TECHNOLOGY NEW SOLUTION
NEW SOLUTION
Canine CAR-T Therapy Development: From early target discovery, CAR design and construction, cell culture, and transfection, to in vitro and in vivo function validation.
LEARN MORE SOLUTION