Overview: Closing the Validation Gap
The Imperative for Empirical Validation
While AI algorithms have revolutionized the identification of tumor neoantigens, the path from "predicted sequence" to "protective immunity" is complex. Genetic mutations are numerous, but only a small fraction result in peptides that are properly processed, stably bound to MHC, and recognized by the TCR. Biological filters like proteasomal cleavage efficiency and HLA binding kinetics create hurdles that computational models alone cannot fully replicate.
Key Preclinical Research Goals
- Validation of Expression: Quantifying mutant protein abundance to ensure sufficient antigen density for recognition.
- Cleavage Accuracy: Verifying correct processing into 8-11mer (MHC I) or 13-25mer (MHC II) peptides.
- MHC-Peptide Stability: Determining the dissociation half-life, a superior predictor of immunogenicity.
- Functional Potency: Assessing the ability to trigger TCR signaling and polyfunctional cytokine release.
- Preclinical Safety: Screening against the human proteome to prevent off-target autoimmune risks.
Featured High-efficiency Evaluation Services
Cell-Based MHC Affinity & Stability Evaluation
Molecular interaction is the bedrock of antigenicity. This service provides a quantitative assessment of the physical bond between neoantigen peptides and the HLA groove. We simulate the competitive cellular environment to ensure predicted binders possess requisite stability.
- Identification of weak/unstable HLA binders.
- Refinement of dissociation rates (k-off).
T Cell In Vitro Induction & Activation System
Functional validation goes beyond binding. Our platform reproduces the immune synapse interaction using human T cells and APCs. By challenging the immune repertoire in vitro, we monitor the actual induction of effector cytokines and cytolytic activity.
- Confirmation of true immunogenicity vs. simple binding.
- Verification of TCR-MHC-peptide specificity.
Humanized PDX Mouse Model Evaluation System
Bridging the gap to clinical reality, we utilize humanized Patient-Derived Xenograft (PDX) models. These models incorporate human immune system components within an in vivo environment, allowing for complex tumor-immune dynamics studies.
- Evaluation of vaccine-induced tumor regression.
- Understanding the impact of the tumor microenvironment (TME).
Evaluation Workflow

Step 1 — Neoantigen Candidate Ingest
Uploading AI-predicted sequences for screening. We support multiple formats including peptide libraries, DNA plasmids, or mRNA construct designs.
Step 2 — Molecular Affinity Screening
Verification of peptide-HLA binding stability. We utilize recombinant proteins to filter out weak binders that cannot form durable immune complexes.
Step 3 — Cellular T Cell Induction
Testing immunogenicity using primary PBMCs. Confirmation of the candidate's ability to trigger specific T cell activation and cytokine secretion.
Step 4 — Preclinical Animal Proof-of-Concept
Advanced validation in humanized PDX models to monitor tumor growth inhibition and systemic immune response in a human-like microenvironment.
Step 5 — Data-Driven Down-Selection
Integrated report providing prioritized candidates for clinical development based on potency, safety, and preclinical efficacy data.
Evaluation Platform Features
Molecule-to-Animal Scope
One-stop validation covering molecular binding, cellular activation, and systemic animal responses to provide a solid data foundation.
Condensed Timelines
Streamlined in vitro protocols and optimized PDX maintenance significantly shorten the antigen verification cycle.
Data-Rich Reporting
Detailed summaries with MHC-binding curves, ELISPOT images, and TGI statistics for clear preclinical decision-making.
Research Insight: Spleen-Targeted Delivery to Remodel "Cold" Environments
Overcoming Tissue Access Barriers with RBC Hitchhiking Strategies
A breakthrough research published in EMBO Molecular Medicine (2023) introduces a transformative RBC-driven spleen targeting strategy designed to remodel the immune "cold" microenvironment of Hepatocellular Carcinoma (HCC). Despite the precision of AI-driven neoantigen identification, the physical delivery of DNA vaccines to professional antigen-presenting cells (APCs) remains a major hurdle due to rapid degradation and off-target sequestration. To address this, researchers developed a cascade delivery system where DNA-encapsulating polymeric nanoparticles are "hitchhiked" onto the surface of preisolated red blood cells (RBCs).
By leveraging the RBCs' natural role as a "blood filter," the vaccines are preferentially dislodged and captured in the spleen—the body’s largest peripheral lymphoid organ—rather than being cleared by the liver. This targeted approach triggers the STING and TLR9 signaling pathways, resulting in a robust burst of neoantigen-specific T-cell immunity. Most significantly, when synergized with anti-PD-1 checkpoint blockade, the strategy achieved complete tumor regression in preclinical models and established long-term immunological memory, effectively preventing tumor recurrence and spontaneous metastasis. This research provides a solid scientific foundation for our evaluation platform, ensuring that predicted candidates translate into potent, protective immunity through systemic validation.
-
Mechanism: DNA vaccine-encapsulating nanoparticles are attached to red blood cells (RBCs), leveraging their filtration dynamics to accumulate in the spleen and promote high-level antigen expression by APCs.
-
Synergy: When combined with anti-PD-1, the RBC-hitchhiking vaccine overcomes the limitations of low tumor mutational burden (TMB) to induce durable tumor-specific memory.
-
Evaluation Significance: Our platform supports high-efficiency validation of neoantigens within these advanced delivery modalities before moving to complex preclinical models.
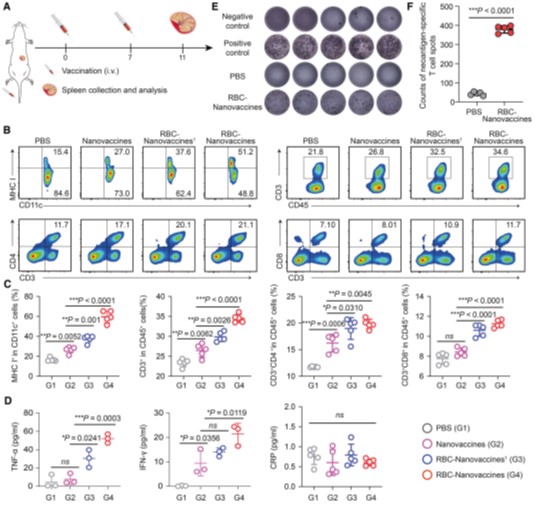
Fig.1 Enhanced neoantigen-specific T-cell response of DNA nanovaccines via RBC-hitchhiking.1,2
