Hematopoietic Stem Cell Transplantation (HSCT) Technology Platform
Creative Biolabs provides a state-of-the-art, integrated hematopoietic stem cell transplantation (HSCT) technology platform specifically designed for preclinical research and translational medicine. Our platform offers a complete suite of services from in vitro Hematopoietic Stem Cell (HSC) isolation and expansion to complex in vivo transplantation modeling and multi-dimensional immune reconstitution analysis. We empower global researchers to evaluate cell therapies, drug candidates, and gene-editing strategies in the context of advanced hematological recovery and immune system development.
Unifying Stem Cell Biology with Preclinical Efficacy
Comprehensive HSC Source & Characterization
Our platform supports various HSC sources, including bone marrow (BM), cord blood (CB), and mobilized peripheral blood (mPB). We employ high-precision immunomagnetic separation and fluorescence-based droplet sorting to enrich for specialized populations such as CD34+, CD133+, and Lin- HSCs. Every cell batch undergoes rigorous in vitro characterization to ensure viability, purity, and functional stemness.
- Platform Strategic Advantages:
- End-to-end integration from cell separation to in vivo efficacy.
- Validated models for Humanized-HSC engraftment and GVHD risk scoring.
- High-resolution monitoring of MRD and multi-lineage immune reconstruction.
Syngeneic vs. Humanized Preclinical HSCT Models
| Parameter | Syngeneic/Allogeneic Mouse Models | HSC-Humanized Mouse Models (CD34+) |
|---|---|---|
| Cell Origin | Donor mouse bone marrow or fetal liver. | Human cord blood, BM, or G-CSF mPB. |
| Immune Reconstitution | Full mouse hematopoietic system recovery. | Human T, B, NK, and myeloid cell development. |
| Therapeutic Testing | Mechanism study; toxicity screening. | Human-specific drug/cell therapy evaluation. |
| Application | Basic hematopoietic research; GVHD modeling. | Preclinical POC for human cell & gene therapies. |
Core Preclinical HSCT Service
Our platform provides a one-stop research suite designed for research institutions, pharmaceutical companies, and translational medicine teams. We offer comprehensive integration across the entire project lifecycle, encompassing everything from HSC source processing and high-purity selection to complex in vivo modeling, immune reconstitution monitoring, and rigorous quality control for preclinical evaluation.
HSC Processing & In Vitro Engineering
- Isolation & Selection: High-purity MACS/FACS enrichment of CD34+, CD133+, and Lin- populations from BM, CB, or mPB.
- Culture & Expansion: Optimized serum-free systems with cytokine cocktails (SCF, TPO, FLT3L) to maintain stemness during expansion.
- Functional Assays: Colony-Forming Unit (CFU) assays and Long-Term Culture-Initiating Cell (LTC-IC) analysis for multi-potency validation.
- Genetic Modification: Gene editing efficiency and off-target evaluation for HSC-based gene therapies.
Advanced Animal Modeling & Engraftment
- Conditioning Protocols: Precise recipient pre-conditioning via X-ray/Gamma irradiation or myeloablative chemotherapy (e.g., Busulfan).
- Transplantation Routes: Professional administration via tail vein, retro-orbital, or specialized intra-bone marrow (IBM) routes.
- Serial Transplantation: Gold-standard primary, secondary, and tertiary transplantation to prove self-renewal capability.
- Homing Assays: In vivo tracking of HSC homing to the bone marrow niche within 24-48 hours post-injection.
Reconstitution & Chimerism Monitoring
- Lineage Analysis: Multi-color FACS monitoring of donor-derived T, B, NK, myeloid, and erythroid cells in peripheral blood and BM.
- Chimerism Detection: High-sensitivity STR, qPCR, and ddPCR for quantifying donor vs. recipient cell ratios (down to 0.1%).
- Kinetic Profiling: Longitudinal mapping of hematopoietic and immune system recovery post-transplant.
- Tissue Pathology: H&E and IHC analysis of lymphoid organs (Spleen, Thymus) to assess structural reconstruction.
Pathology, GVHD & Disease Tracking
- GVHD Evaluation: Standardized clinical scoring and histological assessment of target organs (Skin, Liver, Gut).
- MRD Detection: Molecular residual disease monitoring via qPCR or NGS for leukemic clone tracking post-HSCT.
- MoA Studies: Serum cytokine arrays and immune activation/exhaustion profiling to elucidate therapeutic mechanisms.
- Safety & Release: Pre-clinical QC testing including sterility, mycoplasma, endotoxin, and viability/recovery assays.
Seamless Workflow for Preclinical HSCT Projects
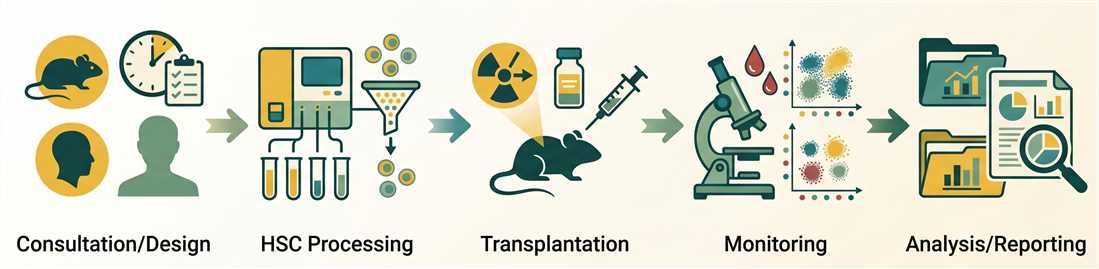
Phase 1 — Project Consultation & Strategic Design
Selection of donor/recipient species and models. We define key endpoints including engraftment kinetics, target chimerism levels, and clinical observation periods for GVHD. All protocols adhere to strict animal welfare and ethical guidelines.
Enabling Technologies for Advanced HSCT Research
Why Choose Creative Biolabs?
Leveraging decades of immunotherapy research, our scientists possess deep insights into HSC biology and complex immune system reconstruction.
Access to a diverse range of validated models, from syngeneic mouse systems to highly sophisticated humanized-HSC mouse platforms.
Our platform achieves exceptional sensitivity in chimerism mapping and MRD detection, providing reliable data for decision-making.
We provide full traceability and rigorous QC for every step, offering a streamlined path from project design to final data delivery.
Research Insight: Adoptive Cell Immunotherapy for R/R EBV-Positive PTLD
Breakthroughs in Off-the-Shelf EBV-Specific T-Cell Therapy
Post-transplant lymphoproliferative disorders (PTLD) driven by Epstein-Barr virus (EBV) represent a life-threatening complication where therapeutic options for relapsed or refractory (R/R) disease are historically limited. Recent advances in adoptive cellular immunotherapy, specifically using EBV-specific cytotoxic T lymphocytes (EBV-CTLs), have significantly redefined the therapeutic landscape.
-
Clinical Efficacy of Tabelecleucel: As a first-in-class allogeneic T-cell therapy, tabelecleucel has demonstrated objective response rates (ORR) of approximately 50-52% in phase III ALLELE trials for both allo-HSCT and SOT recipients. The median duration of response (DOR) reached up to 23 months, offering sustained remission for heavily pretreated patients.
-
Safety and Tolerability: Unlike donor lymphocyte infusions (DLI), third-party off-the-shelf EBV-CTLs exhibit minimal toxicity. Robust clinical data confirm a complete absence of new-onset Graft-versus-Host Disease (GvHD), cytokine release syndrome (CRS), or organ rejection, making them suitable for immunocompromised recipients.
-
Emerging CAR-T Strategies: Beyond CTLs, CD19 CAR-T cell therapy is being explored for R/R PTLD. While promising, researchers must carefully balance lymphodepleting chemotherapy and the modulation of immunosuppression to prevent allograft rejection, necessitating specialized preclinical evaluation models.1
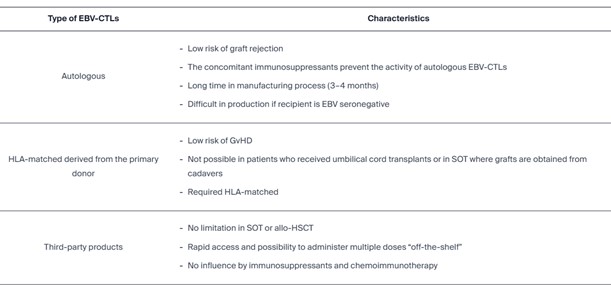
Fig.1 Summary of phenotypic characteristics and functional subsets of EBV‑CTLs used in adoptive transfer.1
Preclinical Development FAQs
Primary transplantation involves injecting HSCs into a first-level recipient. Serial transplantation (secondary or tertiary) involves harvesting donor cells from the primary recipient and injecting them into new mice. This is the definitive in vivo assay to prove long-term self-renewal and stemness of the donor cells.
We use optimized conditioning regimens (e.g., busulfan or sublethal irradiation) tailored to the mouse strain (like NSG or NCG). Additionally, we use high-purity CD34+ selections from cord blood or bone marrow and optimize the dose and route of administration to ensure consistent niche occupancy.
Yes. We utilize high-sensitivity molecular assays such as qPCR for WT1, BCR-ABL, or specific mutant markers. Combined with multiparameter flow cytometry, we can identify very low levels of residual tumor cells among regenerating donor hematopoietic cells.
For mouse-to-mouse HSCT, we typically use CD45.1/CD45.2 congenic strains. For human-to-mouse (humanized) models, we use human-specific anti-CD45 vs. mouse anti-CD45 antibodies to distinguish human hematopoietic reconstruction from the residual mouse system.
Yes. We provide comprehensive pathological assessment of GVHD target organs including skin, liver, and intestine. Our pathologists use standardized scoring systems to quantify lymphocytic infiltration and tissue damage.