Ex Vivo vs In Vivo Delivery
Introduction
In an ex vivo strategy, cells are collected, modified under controlled laboratory conditions, characterized, and returned to the recipient. In an in vivo strategy, a vector or formulation is administered directly so that delivery and genetic modification occur within the body. This distinction shapes target-cell access, vector choice, safety testing, manufacturing, and clinical feasibility. A useful comparison therefore begins with the broader strategies for gene delivery rather than assuming that one route is universally superior.
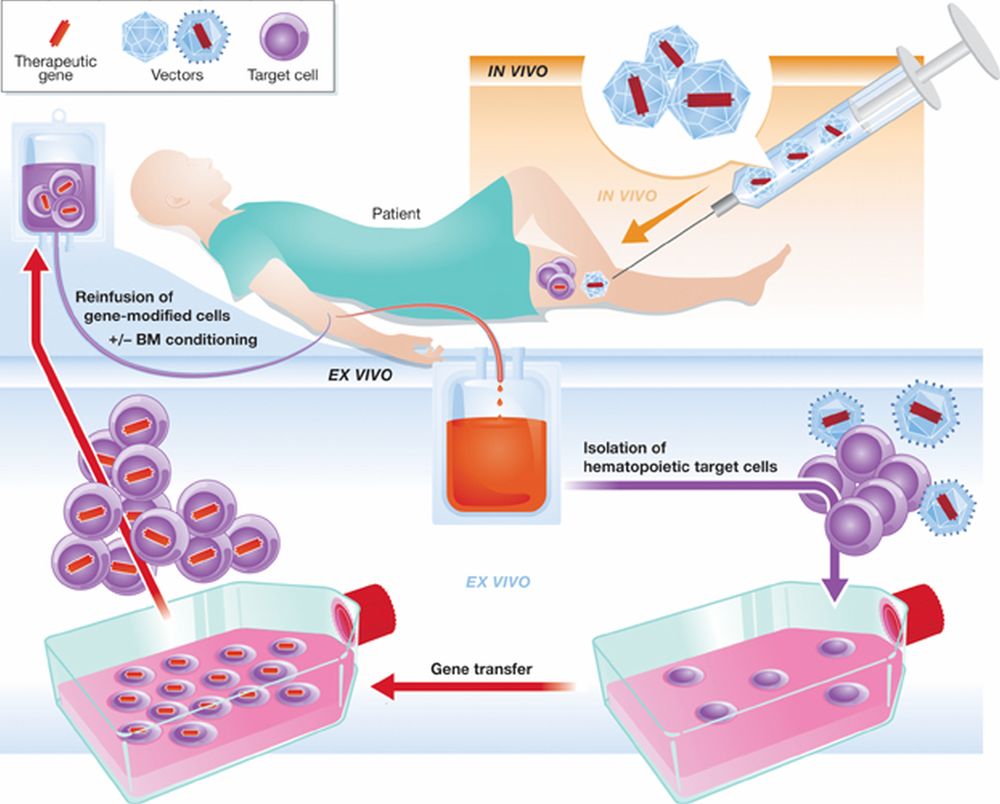 Figure 1. In vivo and ex vivo gene therapy concepts. For the in vivo application of gene-based drugs, the therapeutic gene is introduced directly into the body (e.g. muscle, liver) of the patient, while for ex vivo applications, patient cells are first isolated from the body, genetically modified outside the body and reintroduced into the patient as an autologous transplant (see text for details).1
Figure 1. In vivo and ex vivo gene therapy concepts. For the in vivo application of gene-based drugs, the therapeutic gene is introduced directly into the body (e.g. muscle, liver) of the patient, while for ex vivo applications, patient cells are first isolated from the body, genetically modified outside the body and reintroduced into the patient as an autologous transplant (see text for details).1
Where Genetic Modification Takes Place
The route is defined by the location of cell modification, not simply by whether the payload is viral or non-viral. Both strategies can use gene addition, gene replacement, RNA regulation, or genome editing, but they expose the payload to very different biological and operational environments.
Ex Vivo: Modify, Test, and Return Cells
- Cells are harvested from the patient or a donor. Common starting materials include T cells, natural killer cells, hematopoietic stem and progenitor cells, dendritic cells, and selected stem-cell populations.
- Genetic material is introduced by lentiviral or gammaretroviral transduction, electroporation, transposons, messenger RNA, or CRISPR ribonucleoprotein delivery.
- The modified population can be expanded, enriched, and tested for identity, viability, potency, editing outcome, sterility, and unwanted genomic changes before administration.
- The final product is the engineered cell population, so cell collection, culture conditions, release testing, and chain of identity are integral to the therapy.
In Vivo: Deliver the Payload Directly
- A vector or formulation is administered systemically or locally, such as by intravenous, intrathecal, intracerebral, intramuscular, subretinal, or intratumoral delivery.
- Targeting depends on biodistribution, receptor availability, tissue barriers, vector tropism, promoter control, particle chemistry, and the local immune environment.
- The modified cells cannot usually be isolated and released as a defined product before treatment; therefore, preclinical biodistribution, toxicology, dose-response, and pharmacodynamic studies carry greater weight.
- The administered product is the vector or delivery formulation, while the therapeutic cell population is generated inside the recipient.
Core Differences Between Ex Vivo and In Vivo Delivery
| Decision Dimension | Ex Vivo Delivery | In Vivo Delivery |
|---|---|---|
| Modification site | Outside the body in a controlled manufacturing environment | Inside the body after direct administration |
| Best-suited cells | Cells that can be collected, cultured, manipulated, and reinfused | Cells embedded in organs or tissues that cannot be practically removed |
| Product definition | A genetically modified cell product | A vector, nanoparticle, nucleic acid, or other delivery product |
| Pre-administration control | High: modified cells can be characterized and selected | Limited: cellular outcomes are inferred from validated models and monitored after dosing |
| Dose concept | Often based on viable modified cells and cell attributes | Often based on vector genomes, particles, mass of nucleic acid, or formulation dose |
| Main operational burden | Cell collection, culture, expansion, release testing, logistics | Targeting, biodistribution, tissue exposure, immune response, and systemic safety |
| Typical examples | Engineered T cells and edited hematopoietic stem cells | AAV gene transfer, LNP-delivered RNA or editors, local viral delivery |
| Repeat dosing | May be possible through additional cell manufacture, but conditioning and immunology matter | May be limited by immunity, tissue toxicity, or persistent vector exposure |
Target-Cell Accessibility Is the First Selection Filter
The strongest early question is whether the therapeutically relevant cells can be removed without destroying their function and whether they can be returned to the correct biological niche. This filter often determines the route before detailed vector optimization begins.
When Ex Vivo Is Biologically Practical
- Hematopoietic cells are accessible through blood or marrow collection and can reconstitute durable lineages after reinfusion.
- Immune cells can be isolated and expanded, allowing engineered receptor expression or gene disruption to be measured before dosing.
- Some stem or progenitor cells can serve as carriers of therapeutic genes, although differentiation state, homing, engraftment, and clonal behavior must be controlled. The concept is closely related to the use of a stem cell gene delivery system.
When In Vivo Delivery Is Necessary
- Neurons, retinal cells, cardiomyocytes, skeletal muscle fibers, and hepatocytes usually need to be reached in their native tissue context.
- Diffuse or anatomically protected targets may require systemic exposure or specialized local administration rather than cell removal.
- Tissue architecture may be part of the therapeutic mechanism, making isolated-cell modification biologically incomplete.
- Disease burden may involve many cells across an organ, so therapeutic value depends on coverage, distribution, and expression within the intact tissue.
Vector and Payload Fit for Each Route
Vector choice follows the route, target-cell biology, payload size, desired expression duration, and tolerance for genomic integration. A vector commonly associated with one route may still be used in the other, but the design constraints change substantially.
| Platform | Common Route | Key Strength | Important Limitation | Typical Decision Context |
|---|---|---|---|---|
| Lentiviral vector | Primarily ex vivo | Stable gene transfer in dividing and non-dividing cells | Integration-site and copy-number considerations | Durable expression in engineered immune or hematopoietic cells |
| Gammaretroviral vector | Ex vivo | Efficient stable modification of proliferating cells | Requires careful integration-related safety assessment | Expanded T-cell products and selected cell-manufacturing workflows |
| AAV | Primarily in vivo | Tissue tropism, local or systemic administration, long expression in many non-dividing cells | Limited payload capacity, pre-existing immunity, redosing constraints | Eye, liver, muscle, and central nervous system programs |
| LNP | Primarily in vivo; also ex vivo research | Transient delivery of RNA or gene-editing components without viral genomes | Organ distribution and endosomal escape remain major constraints | Liver-directed RNA or genome-editing delivery |
| Electroporation | Ex vivo | Rapid, non-viral delivery of RNP, RNA, or DNA | Cell stress and viability loss can limit yield | Precise editing of isolated cells |
| Adenoviral/HSV platforms | Often in vivo or local | Large payload capacity and strong transduction in selected tissues | Immunogenicity and expression profile require route-specific control | Vaccination, oncolytic, or localized tissue applications |
For direct tissue modification, engineered capsids and expression cassettes may be evaluated through AAV vector design for gene therapy. For cell-based manufacturing, stable expression is often supported by lentiviral vector development, although vector copy number, insertion-site distribution, transgene regulation, and cell phenotype remain application-specific.
Study Design and Critical Readouts
The two routes require different evidence packages. A strong program measures not only whether the payload is delivered, but also where it acts, how long the effect persists, and whether the modified cellular state remains functional and safe.
Ex Vivo Readouts
- Starting-cell identity, purity, viability, activation state, and fitness.
- Transduction or editing efficiency, allele distribution, vector copy number, and transgene expression.
- Off-target editing, chromosomal rearrangements, integration-site profile, and clonal diversity where relevant.
In Vivo Readouts
- Biodistribution across target and non-target tissues, including persistence of vector genomes or formulation components.
- Tissue-specific transduction or editing, cell-type resolution, and functional expression of the therapeutic payload.
- Innate and adaptive immune responses to capsid, transgene product, delivery lipids, or gene-editing proteins.
Advantages, Limitations, and Translational Trade-Offs
Ex vivo delivery offers control over the cells that become the therapy, whereas in vivo delivery offers access to tissues that cannot be practically manipulated outside the body. The trade-off is therefore control versus reach, not simply complexity versus convenience.
Advantages of Ex Vivo Delivery
- The modified population can be tested before administration.
- Cell phenotype and potency can be linked directly to product-release criteria.
Limitations of Ex Vivo Delivery
- Manufacturing is individualized or donor-dependent and requires controlled cell-processing infrastructure.
- Many solid-organ cell types cannot be harvested and returned effectively.
Advantages of In Vivo Delivery
- The route can reach cells in their native anatomical and physiological environment.
- Systemic delivery may treat widespread disease when sufficient tissue tropism is achieved.
Limitations of In Vivo Delivery
- Cellular modification cannot be fully characterized before dosing.
- Dose scaling from animal models to humans is difficult when receptor biology and tissue distribution differ.
How to Choose Between Ex Vivo and In Vivo Delivery
A route should be selected through a sequence of biological and translational gates. The following questions prevent a program from choosing a familiar vector before defining what the target tissue actually requires.
- Define the therapeutic cell population required for a meaningful biological effect.
- Test whether those cells can be collected, expanded, and returned while retaining function.
- Define the required genetic outcome. Stable integration, episomal expression, transient editing, RNA knockdown, or short-lived protein production lead to different platforms.
- Match payload size, regulatory elements, targeting needs, and vector manufacturability.
- Compare controllability with tissue coverage. Ex vivo workflows favor product characterization; in vivo workflows favor anatomical reach.
- Build route-specific safety assays for cellular quality or for biodistribution, immunity, and organ toxicity.
Research Question vs. Recommended Direction
| Research Situation | Usually Favored Direction | Reasoning |
|---|---|---|
| Autologous T-cell engineering with measurable potency before dosing | Ex vivo | Cells can be isolated, expanded, characterized, and reinfused. |
| Durable correction of hematopoietic stem cells | Ex vivo | Modified stem cells can be assessed before engraftment, although conditioning and clonal follow-up are important. |
| Gene transfer to retina, brain, heart, liver, or skeletal muscle | In vivo | The target cells depend on intact tissue context and cannot be practically removed and returned. |
| Transient liver-directed genome editing with RNA components | In vivo | Systemic formulations can exploit liver uptake; biodistribution and off-target organ exposure remain critical. |
Published Data
Case 1: Ex Vivo CRISPR/Cas9 Gene Editing for Sickle Cell Disease
This 2021 Phase I/II clinical trial evaluated the efficacy of an ex vivo CRISPR/Cas9 gene-editing therapy (CLIMB-121) for severe Sickle Cell Disease (SCD) and β-thalassemia.
- The Goal: To harvest a patient's own CD34+ hematopoietic stem cells from their peripheral blood, and use electroporation in a GMP facility to deliver a CRISPR/Cas9 ribonucleoprotein (RNP) complex. This system specifically targets and disrupts the BCL11A erythroid enhancer. Following myeloablative chemotherapy conditioning, the edited cells are infused back into the patient, aiming to permanently reactivate the production of fetal hemoglobin (HbF).
- The Finding: The therapeutic results were unprecedented. In evaluated SCD patients, the proportion of HbF skyrocketed from a baseline of ~9% to approximately 46% of total hemoglobin, distributing evenly across red blood cells. Clinically, this completely eliminated vaso-occlusive crises (VOCs) in all treated patients, who previously averaged four severe crises per year. The therapy was safe, with no vector-related clonal dominance; severe adverse events were primarily tied to the required chemotherapy preconditioning.
- Practical Takeaway: This pivotal trial conclusively proved the clinical safety and transformative efficacy of ex vivo CRISPR stem cell editing. These exact results provided the direct clinical foundation for Exa-cel (marketed as Casgevy) to make history in late 2023, securing FDA and MHRA approval as the world's very first commercially approved CRISPR-based gene therapy.
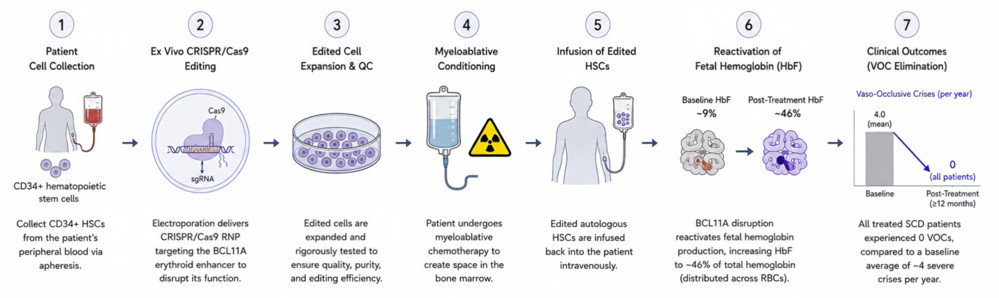 Figure 2. Ex vivo CRISPR/Cas9 gene correction for sickle cell disease.
Figure 2. Ex vivo CRISPR/Cas9 gene correction for sickle cell disease.
Frequently Asked Questions
Q: Is ex vivo delivery always safer than in vivo delivery?
A: No. Ex vivo delivery permits pre-infusion testing of modified cells, but it introduces risks related to cell collection, culture, conditioning, genomic modification, and long-term clonal behavior. In vivo delivery avoids cell manufacturing but requires rigorous control of biodistribution, tissue exposure, immune responses, and off-target effects.
Q: Can AAV be used for ex vivo delivery?
A: Yes, AAV can deliver templates or genetic cargo to isolated cells, especially in genome-editing workflows. However, its most established role is direct in vivo transduction. Ex vivo uses must still consider payload capacity, transduction efficiency, vector dose, and cellular toxicity.
Q: Why are lentiviral vectors commonly used ex vivo?
A: Lentiviral vectors can produce stable transgene expression in dividing and non-dividing cells, making them useful for engineered immune cells and hematopoietic stem cells. Their integrating nature also requires control of vector copy number, insertion profile, transgene regulation, and long-term cellular behavior.
Q: Which route is better for CRISPR delivery?
A: The answer depends on the target cell. Ex vivo delivery is favored when cells can be isolated and edited without losing function. In vivo delivery is required for many organs and may use AAV, LNPs, or other targeted systems. Editor duration, payload size, off-target risk, and tissue specificity must be considered together.
Q: Does in vivo delivery eliminate manufacturing complexity?
A: It reduces patient-specific cell processing but does not eliminate complexity. Vector production, formulation consistency, potency assays, biodistribution studies, dose scaling, immunogenicity assessment, and long-term safety monitoring remain substantial development requirements.
Q: What is the most important early experiment when comparing the two routes?
A: A route-feasibility study should test whether the true therapeutic cell type can be modified at a biologically meaningful level while preserving function. For ex vivo programs, measure recovery, viability, phenotype, and potency. For in vivo programs, measure cell-type-specific distribution, expression or editing, dose response, and non-target tissue exposure.
Overview of What Creative Biolabs Can Provide
Creative Biolabs can support route selection and delivery-system development by connecting target-cell biology with vector design, formulation, gene-editing payload construction, and analytical planning. The appropriate scope depends on whether the project requires a defined engineered cell product or direct modification of cells in their native tissue environment.
| Research Need | Related Creative Biolabs Support | How It Connects to the Current Resource Topic |
|---|---|---|
| Select and construct a viral delivery platform | Custom Viral Vector Development | Supports route-specific vector selection, cassette design, and construction for direct or cell-based delivery. |
| Develop an AAV system for direct tissue delivery | Adeno-associated Virus Vector Development Service | Connects capsid, promoter, payload, and tissue-targeting choices for in vivo programs. |
| Improve AAV tissue or cell targeting | Tissue/Cell Specific Targeting Advanced Adeno-Associated Virus Vector Service | Addresses biodistribution and cell-type selectivity, which are central limitations of in vivo delivery. |
| Formulate non-viral RNA or editing cargo | Lipid Nanoparticle (LNP) | Supports development of LNP-based delivery where transient in vivo payload exposure is desired. |
| Construct delivery agents for gene editing | CRISPR related Delivery Agent Construction Services | Links editing modality with viral or non-viral delivery design for ex vivo or in vivo use. |
| Develop CRISPR cargo in an LNP format | CRISPR assisted Lipid Nanoparticle (LNP) Formulation Service | Supports transient in vivo delivery of RNA and genome-editing components. |
| Explore cell carriers for ex vivo strategies | Development of Stem Cell as Gene Delivery System | Relates to collection, modification, characterization, and return of engineered stem or progenitor cells. |
For a route-specific development plan, contact us today to discuss the therapeutic cell type, payload, target tissue, required expression duration, and translational stage.
References
- Kaufmann K B, Büning H, Galy A, et al. Gene therapy on the move. EMBO molecular medicine, 2013, 5(11): 1642-1661. https://doi.org/10.1002/emmm.201202287 Distributed under Open Access license CC BY 4.0, with modification.
- Frangoul H, Altshuler D, Cappellini M D, et al. CRISPR-Cas9 gene editing for sickle cell disease and β-thalassemia. New England Journal of Medicine, 2021, 384(3): 252-260. 10.1056/NEJMoa2031054