RNAi Therapy Introduction
Introduction
RNA interference (RNAi) therapy uses sequence-programmed RNA molecules to reduce the expression of disease-relevant genes at the messenger RNA level. Unlike permanent genome editing, RNAi generally produces a reversible pharmacological effect whose magnitude and duration depend on sequence chemistry, intracellular exposure, target turnover, and tissue delivery. This resource explains the therapeutic logic of RNAi, the major molecular formats, delivery options, translational readouts, and limitations that shape development.
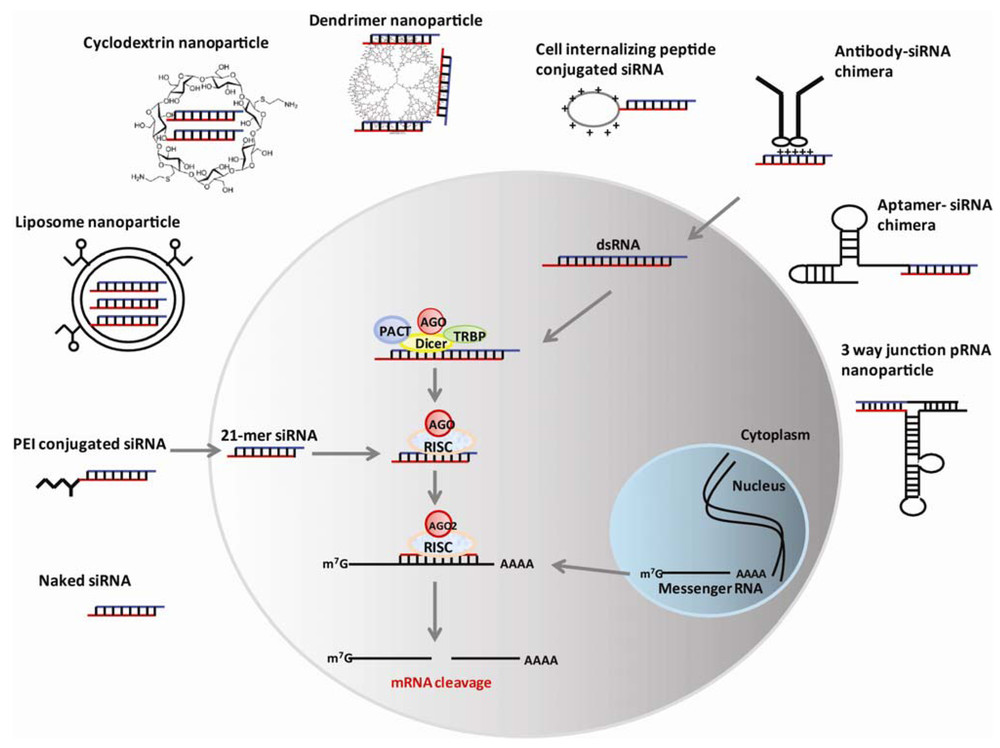 Figure 1. The mechanism and delivery strategies for RNA interference.1
Figure 1. The mechanism and delivery strategies for RNA interference.1
Therapeutic Scope of RNA Interference
RNAi is most useful when disease biology can be modified by lowering a transcript rather than replacing a missing protein. The approach can address toxic gain-of-function proteins, overactive signaling nodes, pathogenic viral RNAs, and metabolic targets whose partial suppression is beneficial.
What RNAi changes—and what it does not
- RNAi acts after transcription, so genomic DNA is not intentionally cut or rewritten.
- The pharmacodynamic effect is targeting knockdown, which may be partial rather than complete and can be renewed by repeat dosing.
- Therapeutic success requires sufficient guide-loaded RNA-induced silencing complex (RISC) in the relevant cell type, not merely high total tissue RNA.
- Because RNAi lowers both mutant and wild-type transcripts when sequences are shared, allele selectivity must be designed deliberately when normal protein is required.
| Disease logic | Why RNAi may fit | Key boundary |
|---|---|---|
| Toxic gain of function | Lowering the causative transcript may reduce production of a harmful protein | Residual wild-type function and irreversibility of tissue damage must be considered |
| Metabolic overactivity | Partial suppression can reset a pathway without eliminating the gene | Dose-response windows and compensatory pathways may limit benefit |
| Viral infection | Conserved viral RNA regions can be targeted sequence-specifically | Viral escape, delivery to infected cells, and innate immune activation remain concerns |
| Oncology | Transient knockdown can test or modulate oncogenic dependencies | Tumor heterogeneity and extrahepatic delivery are major barriers |
Therapeutic RNAi Modalities
The term RNAi therapy covers chemically synthesized oligonucleotides and vector-encoded precursors. These formats enter the pathway at different points and therefore differ in onset, persistence, controllability, and safety assessment.
Synthetic siRNA
A small interfering RNA (siRNA) duplex is delivered as a defined drug substance. Chemical stabilization can protect it from nucleases, tune strand selection, reduce innate immune sensing, and extend tissue exposure. Because the duplex itself is not replicated, activity wanes as active RISC complexes turn over and cells divide.
Vector-expressed shRNA or miRNA scaffolds
Short hairpin RNA (shRNA) and engineered microRNA precursors are transcribed inside target cells and processed into guide RNAs. Viral delivery may provide durable silencing in slowly dividing tissues, but expression level, promoter behavior, saturation of endogenous RNA-processing machinery, and vector-specific risks require careful control. Long-term studies often benefit from deliberate AAV-based RNAi vector design.
| Format | Typical duration | Strength | Primary development risk |
|---|---|---|---|
| Chemically modified siRNA | Weeks to months, depending on tissue and chemistry | Defined composition and adjustable repeat dosing | Delivery, endosomal escape, off-target seed effects |
| shRNA expression cassette | Potentially long-term | Sustained intracellular production | Overexpression toxicity, vector persistence, limited reversibility |
| Artificial miRNA scaffold | Potentially long-term | Often better processing control than simple shRNA | Context-dependent processing and guide abundance |
| Dicer-substrate RNA | Often transient | Can enhance processing in selected systems | More complex structure-activity relationships |
Delivery Determines the Reach of RNAi Therapy
RNA molecules are large, polyanionic, and vulnerable to degradation. They do not freely cross cell membranes, and cellular uptake does not guarantee cytosolic release. Delivery therefore determines which organs, cell populations, and diseases are realistically addressable.
Conjugate-based delivery
Ligands can direct siRNA to receptors enriched on a target cell. The clinically validated example is N-acetylgalactosamine targeting the asialoglycoprotein receptor on hepatocytes. Other ligands, peptides, and antibodies are being explored, but receptor abundance, internalization, trafficking, and species differences must be quantified. The broader strategy is summarized under ligand-targeted RNAi delivery.
Nanoparticle and excipient-based delivery
Lipid and polymeric systems can protect RNA, promote uptake, and enable endosomal escape. Formulation composition affects particle size, encapsulation, biodistribution, tolerability, and manufacturability. Potent particles may still show liver or spleen bias, and apparent uptake in non-target cells may not translate into productive cytosolic delivery.
Local and vector-mediated delivery
- Local administration can reduce systemic exposure for ocular, pulmonary, dermal, or central nervous system applications, but distribution within the tissue may be uneven.
- Viral vectors can express RNAi triggers in situ, supporting durable knockdown but requiring vector biodistribution, expression stability, and immune risk analysis.
- Extracellular vesicles and exosome-inspired systems are under active investigation, although loading consistency, targeting, and scalable characterization remain development challenges.
Building a Translational RNAi Program
A credible program connects target biology, sequence selection, delivery, pharmacology, and safety in one evidence chain. Strong in vitro knockdown alone is not sufficient because intracellular concentration, cell state, transcript turnover, and animal-to-human delivery can change the outcome.
| Development question | Recommended evidence | Decision value |
|---|---|---|
| Is the transcript causally linked to disease? | Genetic validation, rescue experiments, orthogonal knockdown reagents | Reduces the risk of advancing a correlated but non-causal target |
| Does knockdown occur in the intended cells? | Cell-resolved RNA/protein readouts, tissue distribution, uptake and endosomal escape assays | Separates bulk tissue exposure from productive target engagement |
| Is the effect sequence-specific? | Mismatch controls, transcriptome profiling, seed-family analysis | Distinguishes on-target pharmacology from off-target repression |
| Is the exposure durable enough? | Time-course PK/PD, guide-strand quantification, RISC loading where feasible | Supports dosing interval and formulation selection |
| Is the therapeutic window acceptable? | Cytokines, complement, liver markers, histopathology, hybridization-dependent and independent toxicity endpoints | Links efficacy to dose-limiting mechanisms |
Analytical development should include drug identity, purity, concentration, stability, and biologically meaningful nucleic acid potency. Transcript-level pharmacodynamics can be complemented by RNA profiling to identify pathway correction and unintended expression changes.
Therapeutic Applications and Current Boundaries
Clinical progress has been strongest in liver-directed indications because hepatocyte-targeted conjugates and lipid nanoparticles provide reproducible exposure. The wider promise of RNAi depends on extending delivery to tumors, immune cells, muscle, lung, and the central nervous system without losing safety or manufacturability.
Rare and metabolic diseases
RNAi can lower a well-defined pathogenic or pathway-driving liver transcript. Biomarkers are often measurable, which supports dose selection and proof of mechanism.
Cardiovascular risk modification
Long-lived hepatic knockdown can reduce circulating proteins that regulate lipid metabolism. Long-term safety and treatment adherence remain central.
Cancer
RNAi offers access to intracellular targets, but heterogeneous tumor perfusion, stromal barriers, and delivery to metastatic sites limit consistency.
Infectious disease
Highly conserved pathogen sequences are conceptually attractive, although mutation, intracellular localization, and rapid disease kinetics complicate development.
Neurological disease
Local administration or vector expression can bypass systemic barriers, but anatomical distribution, neuronal subtype targeting, and reversibility are critical constraints.
Published Data
Case 1: Inclisiran (RNAi) for Heterozygous Familial Hypercholesterolemia
This 2020 Phase III, double-blind, randomized controlled trial (ORION-9), published in the New England Journal of Medicine, evaluated the efficacy and safety of inclisiran in 482 adult patients with heterozygous familial hypercholesterolemia.
- The Goal: To utilize inclisiran—a small interfering RNA (siRNA) drug—to inhibit the synthesis of PCSK9 protein in the liver. By binding and degrading PCSK9 mRNA, the therapy allows for increased recycling and expression of low-density lipoprotein (LDL) receptors on the liver surface, which subsequently clears more LDL cholesterol (LDL-C) from the bloodstream.
- The Finding: Patients received subcutaneous injections of either inclisiran (300 mg) or a placebo on days 1, 90, 270, and 450. By day 510, the inclisiran group achieved a remarkable placebo-adjusted reduction in LDL-C levels of 47.9%, alongside a 78.3% drop in PCSK9 protein levels. The drug demonstrated an excellent safety profile, with tolerability similar to the placebo and no new safety signals reported.
- Practical Takeaway: This landmark trial proves that RNA interference (RNAi) technology can be successfully scaled from rare genetic disorders to broad, common population diseases like hypercholesterolemia. Because inclisiran requires only two subcutaneous injections per year (after the initial loading dose), it represents a massive leap forward in patient compliance and convenience compared to daily oral statins or monthly monoclonal antibody injections.
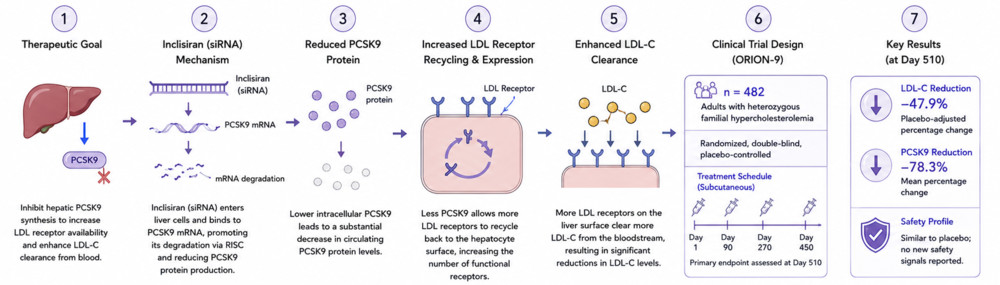 Figure 2. RNAi-based therapeutic approach for treating heterozygous familial hypercholesterolemia.
Figure 2. RNAi-based therapeutic approach for treating heterozygous familial hypercholesterolemia.
Frequently Asked Questions
Q: Is RNAi therapy the same as gene editing?
A: No. RNAi usually reduces gene expression by directing post-transcriptional silencing of RNA, whereas gene editing intentionally changes genomic DNA. RNAi effects are generally reversible and exposure-dependent.
Q: How long does an RNAi therapeutic remain active?
A: Duration varies from days to months depending on chemistry, tissue retention, cell turnover, RISC stability, and whether the trigger is dosed as an oligonucleotide or expressed from a vector.
Q: Why are many approved siRNA therapies liver-directed?
A: Hepatocytes are accessible to clinically validated GalNAc conjugates and lipid nanoparticles, and many liver-derived targets have measurable circulating biomarkers. Efficient extrahepatic delivery remains harder.
Q: Can RNAi distinguish a mutant allele from the normal allele?
A: It can when the disease allele contains a unique sequence, such as a linked variant or mutation that permits selective guide design. When sequences are shared, total transcript knockdown is more likely.
Q: What are the major safety risks?
A: Important risks include unintended seed-mediated gene repression, innate immune activation, delivery-system toxicity, exaggerated on-target pharmacology, and tissue accumulation after repeat dosing.
Q: Which readout is most important for an RNAi study?
A: A strong package measures guide exposure, target RNA reduction, target protein reduction, pathway or phenotype correction, and safety over time. No single readout is sufficient by itself.
Overview of What Creative Biolabs Can Provide
To accelerate RNAi therapeutic development, Creative Biolabs provides end-to-end capabilities spanning target sequence screening, formulation strategy, analytical quality control, in vivo efficacy evaluation, and toxicology testing. Our support model is stage-responsive: we calibrate our focus to align with the critical path of each program—be it lead optimization, pharmacokinetic/pharmacodynamic (PK/PD) improvement, or IND-enabling study preparation.
| Research Need | Related Creative Biolabs Support | How It Connects to the Current Resource Topic |
|---|---|---|
| Integrated RNAi candidate development | RNAi Therapy Development Service | Connects target selection, RNA format, delivery, and preclinical evaluation. |
| Tissue-appropriate delivery | Delivery Method Development Service for RNAi | Matches formulation or administration strategy to target-cell access. |
| Receptor-directed uptake | Ligand-targeted Delivery for RNAi | Supports conjugate concepts for cell-selective internalization. |
| Conjugate optimization | Custom Oligonucleotide Conjugation Service | Links siRNA to targeting or exposure-modifying moieties. |
| Exposure and disposition | Oligonucleotide Drug DMPK Service | Evaluates distribution, persistence, and PK/PD relationships. |
| Safety package | Oligonucleotide Drug Toxicity Assessment Service | Assesses sequence-, chemistry-, and delivery-associated risks. |
Researchers with a defined target, tissue, or development question can contact us today to discuss a fit-for-purpose RNAi strategy.
References
- Zhou J, Shum K T, Burnett J C, et al. Nanoparticle-based delivery of RNAi therapeutics: progress and challenges. Pharmaceuticals, 2013, 6(1): 85-107. https://doi.org/10.3390/ph6010085 Distributed under Open Access license CC BY 4.0, with modification.
- Raal F J, Kallend D, Ray K K, et al. Inclisiran for the treatment of heterozygous familial hypercholesterolemia. New England Journal of Medicine, 2020, 382(16): 1520-1530. 10.1056/NEJMoa1913805