Viral Vector Selection by Target Tissue
Introduction
Target tissue is one of the strongest determinants of viral vector selection. AAV, lentivirus, and adenovirus differ not only in payload capacity and expression duration, but also in how they enter cells, distribute after administration, trigger immunity, and respond to capsid, envelope, or promoter engineering. This Resource explains how tissue/cell specific AAV targeting and related lentiviral or adenoviral strategies can be evaluated when the central question is where the vector must act.
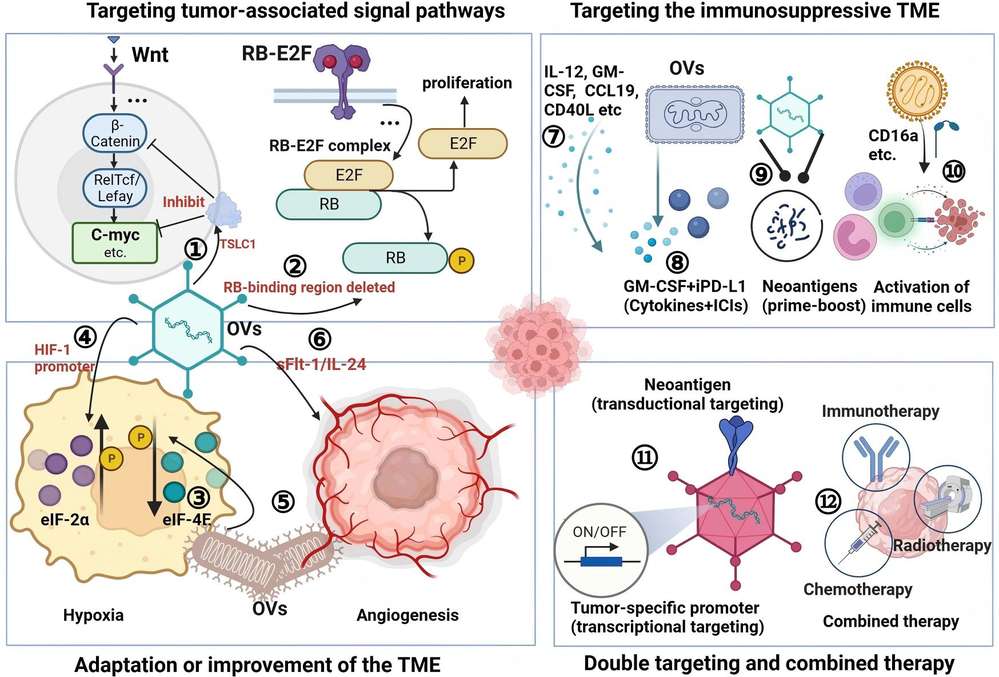 Figure 1. Mechanism for targeting and oncolysis of OVs. Oncolytic viruses (OVs) target dysfunctional signaling pathways.1
Figure 1. Mechanism for targeting and oncolysis of OVs. Oncolytic viruses (OVs) target dysfunctional signaling pathways.1
Why Target Tissue Changes Vector Choice?
A vector selected for liver delivery may fail in lung, retina, muscle, or central nervous system studies because each tissue imposes distinct barriers. These include vascular access, extracellular matrix density, epithelial surfaces, immune surveillance, cell turnover, receptor availability, and feasible administration route. Tissue selection should therefore be treated as a biological design problem rather than a final label added after vector construction.
| Tissue consideration | Why it matters | Vector-selection consequence |
|---|---|---|
| Cell division rate | Dividing cells can dilute episomal genomes; non-dividing cells may support longer AAV expression. | Stable integration may be preferred for expanding cell populations, while AAV is attractive in post-mitotic tissues. |
| Physical access | Blood-brain barrier, mucus, extracellular matrix, or vascular fenestration can limit vector contact. | Route and local administration may matter as much as capsid or envelope choice. |
| Receptor and co-receptor expression | Vector entry depends on cell-surface interactions that vary by species and disease state. | Capsid modification, pseudotyping, or retargeting may be needed. |
| Immune environment | Liver, muscle, lung, and tumors differ in innate sensing, resident immune cells, and inflammation. | Dose, serotype, vector generation, and promoter design must be evaluated with immune readouts. |
| Functional endpoint | Some tissues require broad transduction; others require a small corrected cell population. | The required transduction threshold should be defined before choosing the vector. |
Vector Tropism Is Built from Multiple Control Layers
Tropism is often discussed as if it were a single property of a viral capsid or envelope, but practical tissue targeting is layered. Entry, intracellular trafficking, genome persistence, promoter activity, and immune clearance all shape the final expression pattern. A vector may enter a tissue but express poorly, or express strongly in off-target cells after broad entry.
Capsid, envelope, or fiber interactions
AAV tropism can be modified through serotype choice, rational capsid mutation, peptide insertion, or directed evolution. Lentiviral vectors use envelope glycoproteins, so lentiviral glycoprotein optimization becomes central when the target cells are neurons, hepatocytes, lung cells, myocytes, or other defined populations. Adenoviral tropism can be changed through capsid, fiber, knob, peptide, or ligand-retargeting strategies.
Transcriptional targeting
Entry does not guarantee useful specificity. AAV, lentiviral, and adenoviral vectors can all use promoters or regulatory elements to limit expression after delivery. Specific promoter driven targeting is particularly useful when the vector can reach multiple tissues but the readout should occur only in one cell lineage or disease state.
Post-transcriptional and microenvironmental control
miRNA target sites, hypoxia-response elements, inflammation-responsive systems, and inducible regulatory circuits can further refine expression. These controls are especially valuable in tumors, immune-rich tissues, and models where off-target expression could obscure mechanism or create safety signals.
Route, Dose, and Biological Barriers
The same vector can produce different tissue patterns after systemic, local, intrathecal, intravitreal, intramuscular, intratumoral, or ex vivo administration. Route determines which anatomical barriers the vector encounters first and which immune compartments are activated. Dose changes both efficacy and toxicity, so tissue selection should include a dose-response plan rather than a single high-dose test.
| Route or barrier | Typical selection issue | Practical readout |
|---|---|---|
| Systemic delivery | Broad biodistribution and liver exposure may dominate the profile. | Vector genomes and expression across target and off-target organs. |
| Intrathecal or CNS-directed delivery | CNS compartment access, neuronal versus glial expression, and species differences are critical. | Cell-type expression mapping, neuroinflammation markers, and functional rescue. |
| Intravitreal or subretinal delivery | Retinal layer access and immune privilege affect expression pattern. | Retinal cell-type expression, ocular inflammation, and visual-function assays. |
| Intramuscular delivery | Local spread, muscle fiber transduction, and immune recognition shape durability. | Expression area, fiber-type specificity, serum biomarkers, and histology. |
| Intratumoral delivery | Tumor heterogeneity and extracellular matrix can restrict spread. | Spatial distribution, tumor-cell killing, immune infiltration, and bystander effects. |
Target-Tissue Selection Matrix
A tissue-focused matrix helps compare vectors without overgeneralizing. The examples below are not absolute rules; they are starting points for deciding which vectors deserve experimental comparison in a given model.
| Target tissue or model | Vector options to compare | Main design question |
|---|---|---|
| Retina and ocular tissues | AAV serotypes or engineered AAV; adenovirus for transient research models | Can the vector reach the correct retinal layer with acceptable inflammation and cassette size? |
| Central nervous system | AAV capsids, lentiviral pseudotypes, adenoviral retargeting in selected models | Which cell type must express the payload, and does the route reach that cell type? |
| Liver | AAV, adenovirus, lentiviral hepatocyte pseudotyping in research models | Is broad hepatocyte expression beneficial, and how will liver immunity and dose be managed? |
| Skeletal or cardiac muscle | AAV muscle-tropic variants, adenoviral muscle targeting, lentiviral myocyte pseudotyping | Does the study require local or systemic distribution and long-term expression? |
| Lung airway | AAV or lentiviral pseudotypes; adenovirus in transient or vaccine contexts | Can the vector cross mucus and apical barriers while minimizing inflammation? |
| Solid tumors | Adenovirus, lentivirus, AAV, or hybrid strategies | Is the goal direct tumor-cell transduction, immune stimulation, or local payload production? |
Interpreting Tissue Tropism Data Carefully
Tropism data are useful only when the model, route, and assay are clear. A vector that appears liver-tropic after systemic administration may simply be exposed to liver at a higher level than other tissues. A vector that transduces neurons after direct injection may not cross barriers after systemic dosing. A vector that gives strong reporter expression may still have broad genome distribution with expression restricted by the promoter. These distinctions matter because target-tissue selection is often a balance between where the vector goes and where the payload is allowed to act.
| Data type | What it can show | What it cannot prove alone |
|---|---|---|
| Vector genome copies | Where vector DNA is detectable after dosing. | Which cell type expresses the payload or whether expression is functional. |
| Reporter expression | Where the promoter and vector together produce visible signal. | Whether genome distribution is restricted or whether therapeutic payload behaves similarly. |
| Cell-type markers | Which cell populations express the payload. | Long-term durability, immune consequences, or whole-organ function. |
| Functional assay | Whether the intended biology changes. | Whether the effect is target-cell specific without supporting localization data. |
Designing Tissue Studies across Species and Disease States
Target-tissue selection becomes more difficult when moving from cultured cells to animals or from healthy models to diseased tissue. Receptor abundance, vascular permeability, extracellular matrix composition, inflammation, and cell turnover can change during disease. A vector selected in healthy animals may underperform in fibrotic, inflamed, degenerating, or tumor-bearing tissue. Conversely, disease-associated receptor expression may create an opportunity for targeted delivery that is not visible in normal models.
Species translation also requires caution. AAV serotype patterns, adenoviral receptor use, and lentiviral pseudotype performance can differ between mouse, non-human primate, and human cells. For this reason, tissue-directed projects often benefit from a layered validation strategy:
- Initial screening in accessible models
- Confirmation in relevant human cell or organoid systems
- Biodistribution or safety evaluation in the most informative in vivo model available for the research question.
When to Revisit the Initial Tissue Choice?
Tissue-directed vector plans should be revisited when biodistribution, expression mapping, or functional assays disagree. If vector genomes are present but expression is weak, the problem may involve promoter activity, intracellular processing, or payload toxicity. If expression is strong but function is weak, the vector may be reaching the wrong cell subtype or too small a fraction of the target tissue. If off-target organs show signal, dose, route, capsid, envelope, or transcriptional control may need to be redesigned. Reassessment should be based on mapped evidence rather than a general assumption that the vector failed.
Timing also matters. Some tissues show early expression followed by immune clearance, while others require longer observation to detect functional correction. Sampling only one time point can therefore distort vector selection. A tissue-focused design should include early biodistribution, peak expression, and durability time points whenever feasible, especially for studies intended to inform later translational work.
Documenting the Final Tissue Rationale
The final tissue-selection rationale should record why the chosen vector, route, promoter, and dose were selected and which alternatives were rejected. This documentation is valuable for internal review, manuscript methods, and later troubleshooting. It also prevents future teams from repeating a rejected design when the original reason was tissue access, not vector production quality.
Published Data
Case 1: Engineering AAV Capsids for Targeted Delivery to Cardiomyocytes
This study addresses a core challenge in cardiac gene therapy: achieving precise targeting of cardiomyocytes while minimizing off-target uptake in organs like the liver. Using in vivo AAV2 peptide display library screening within a mouse model of pressure overload-induced cardiac hypertrophy, researchers identified two novel AAV capsid variants: AAV2-THGTPAD and AAV2-NLPGSGD. Both variants demonstrated significantly enhanced transduction efficiency in cardiomyocytes compared to the parental AAV2 serotype. Remarkably, they also outperformed the reference AAV9 serotype in cardiac tropism while substantially reducing off-target accumulation in the liver and non-cardiac cells.
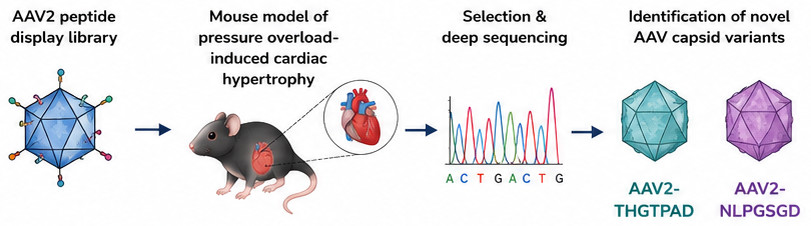 Figure 2. Rational design of AAV capsid variants for cardiac muscle targeting.
Figure 2. Rational design of AAV capsid variants for cardiac muscle targeting.
In therapeutic applications, these novel variants mediated superior anti-hypertrophic effects even at low vector doses, exhibiting an excellent targeting signal-to-noise ratio. Furthermore, the structural modifications positively impacted immunogenicity. Sera from mice treated with these new variants showed weaker neutralizing capabilities, indicating enhanced immune evasion. Ultimately, AAV2-THGTPAD and AAV2-NLPGSGD emerged as highly promising, heart-directed gene therapy tools, offering superior specificity and therapeutic efficacy for in vivo cardiomyocyte transduction compared to the standard AAV9.
Frequently Asked Questions
Is AAV always the best vector for tissue targeting?
No. AAV serotypes and engineered capsids are valuable for many tissue-directed studies, but target tissue access also depends on route, dose, species, disease state, receptor expression, and promoter design. Lentiviral pseudotyping or adenoviral retargeting may be more relevant in some models.
How does target tissue influence promoter choice?
A tissue-relevant promoter can reduce off-target expression even when vector entry is broad. Promoter choice should be evaluated together with capsid or envelope tropism, because entry specificity and expression specificity are different control layers.
Why do mouse tropism data not always translate to humans?
Species differences in receptor expression, immune status, tissue architecture, vector dose, and route can change tropism. Mouse data are useful for ranking candidates, but human cells, organoids, or relevant large-animal models may be needed for translational confidence.
Which tissues are difficult for viral vector delivery?
Barriers vary by route, but commonly difficult contexts include central nervous system compartments, skeletal and cardiac muscle at systemic scale, lung airway epithelium, fibrotic liver, solid tumors, and tissues with strong pre-existing immunity or poor vascular access.
What readouts should be included in tissue-directed vector selection?
Key readouts include target-tissue vector genome copies, cell-type-specific expression, off-target biodistribution, histology, immune activation, dose response, functional rescue, and durability. A single reporter image is not sufficient for tissue selection.
Overview of What Creative Biolabs Can Provide
Creative Biolabs can support viral-vector selection projects by connecting the biological objective with vector design, targeting strategy, expression control, and safety-related readouts. The support below is selected from the Gene Therapy service structure because each item directly relates to AAV, lentiviral, adenoviral, or tissue-directed vector decision-making rather than general promotion.
| Research Need | Related Creative Biolabs Support | How It Connects to the Current Resource Topic |
|---|---|---|
| AAV tissue or cell targeting strategy | Tissue/Cell Specific Targeting Advanced Adeno-Associated Virus Vector Service | Directly supports target-tissue planning through AAV capsid and targeting considerations. |
| AAV capsid engineering | AAV Capsid Modification | Connects tropism modification with delivery efficiency and immune-escape questions. |
| Tissue-restricted AAV expression | Specific Promoter Driven Targeting of AAV Vector | Adds transcriptional specificity when vector entry alone is insufficient. |
| Lentiviral neuronal targeting | Pseudotyping of Lentiviral Vector for Targeting Neuronal Cell | Relevant for tissue-focused studies using envelope selection to bias cell entry. |
| Lentiviral hepatocyte targeting | Pseudotyping of Lentiviral Vector for Targeting Hepatocytes | Supports hepatocyte-focused lentiviral pseudotyping considerations. |
| Adenoviral liver targeting | Liver-targeting Adenovirus Vector Construction Service | Useful when adenoviral biology is desired and liver-directed delivery is the model focus. |
| Adenoviral neural targeting | Neurons-targeting Adenovirus Vector Construction Service | Connects adenoviral retargeting strategy with neuronal cell or tissue applications. |
For projects where vector choice remains uncertain, researchers can contact us today to discuss the target tissue, payload, model system, and readout plan before committing to construction.
References
- Wang S, Liang B, Wang W, et al. Viral vectored vaccines: design, development, preventive and therapeutic applications in human diseases. Signal transduction and targeted therapy, 2023, 8(1): 149. https://doi.org/10.1038/s41392-023-01408-5 Distributed under Open Access license CC BY 4.0, with modification.
- Rode L, Bär C, Groß S, et al. AAV capsid engineering identified two novel variants with improved in vivo tropism for cardiomyocytes. Molecular Therapy, 2022, 30(12): 3601-3618. 10.1016/j.ymthe.2022.07.003